At a glance
Nasopharyngeal radium irradiation (NRI) was a radiation treatment used from the 1940s to the 1960s. This treatment was discontinued because alternative treatments were developed and there was concern about possible radiation carcinogenesis. CDC has undertaken a number of activities that will provide help for people who have had NRI treatment.
The basics
From 1940 through the 1960s, NRI was used to treat hearing loss, chronic otitis, and other conditions among children. It was also used by the military to treat aerotitis media (discomfort in middle ear due to changes in pressure) in submariners and aviators. Before 1950, NRI was one of several radiation treatments used to treat benign conditions.
Other treatments included the use of external x-irradiation to treat
- hearing loss
- acne
- tinea capitis (fungal infection on the scalp)
- enlarged adenoids
- enlarged thymus
- topical radon and radium to treat hemangiomas (benign tumors).
This treatment was discontinued because alternative treatments were developed (T-tubes and better antibiotics) and because of concern about forming cancer.
What CDC is doing
CDC undertook a number of activities to provide help for people who have had NRI treatment.
Through various medical journals, we alerted physicians and other health care practitioners about possible risks from NRI. This work can be seen in the Journal of the American Medical Association – April 17, 1996.
Along with a number of co-sponsors, CDC produced a nationwide satellite medical education conference on NRI (September 1996).
This provided physicians and health care workers throughout the nation with information about the potential risks from NRI. The conference also provided training in how to conduct a thorough examination of the head and neck.
Common Questions
NRI was used for areas in which surgeons could not operate. It did not require general anesthesia or hospitalization. NRI was felt to be a safer treatment than conventional x-ray.
Primary Conditions
- Hearing loss
- Ear pain due to changes in pressure
- Aerotitis media
- Middle ear barotrauma
Other Conditions
- Sinusitis (sinus infection)
- Asthma
- Repeated viral and bacterial infections
- Recurrent tonsillitis
- Recurrent acute otitis media (repeat middle ear infection)
- Chronic otitis media (chronic ear infection)
An estimated 500,000 to 2 million civilians were treated. Treatments began as early as 1940 and continued until the mid to late 1960s. The majority of these civilians were children at the time of treatment. Most of the patients were born before 1960. The peak use of NRI was most likely among children who were born between 1940 and 1950. More than 8,000 World War II servicemen also received NRI.
The goal of treating an individual with NRI was to reduce swollen tissues surrounding the opening of the eustachian tubes. It was thought that reducing the amount of swollen tissue would allow the ears to drain. This was thought to prevent chronic ear infections that could lead to hearing loss. Typical treatments lasted from 6 to 12 minutes and were commonly repeated at 2- to 3-week intervals. A total of 3 treatments were administered. Occasionally a second course of 3 treatments was given.
Radiation doses among adults to nearby organs were estimated on the basis of 50 mg of radium sulfate. Doses were administered in two 0.5-mm platinum capsules for 12–60 minutes per session for three sessions.
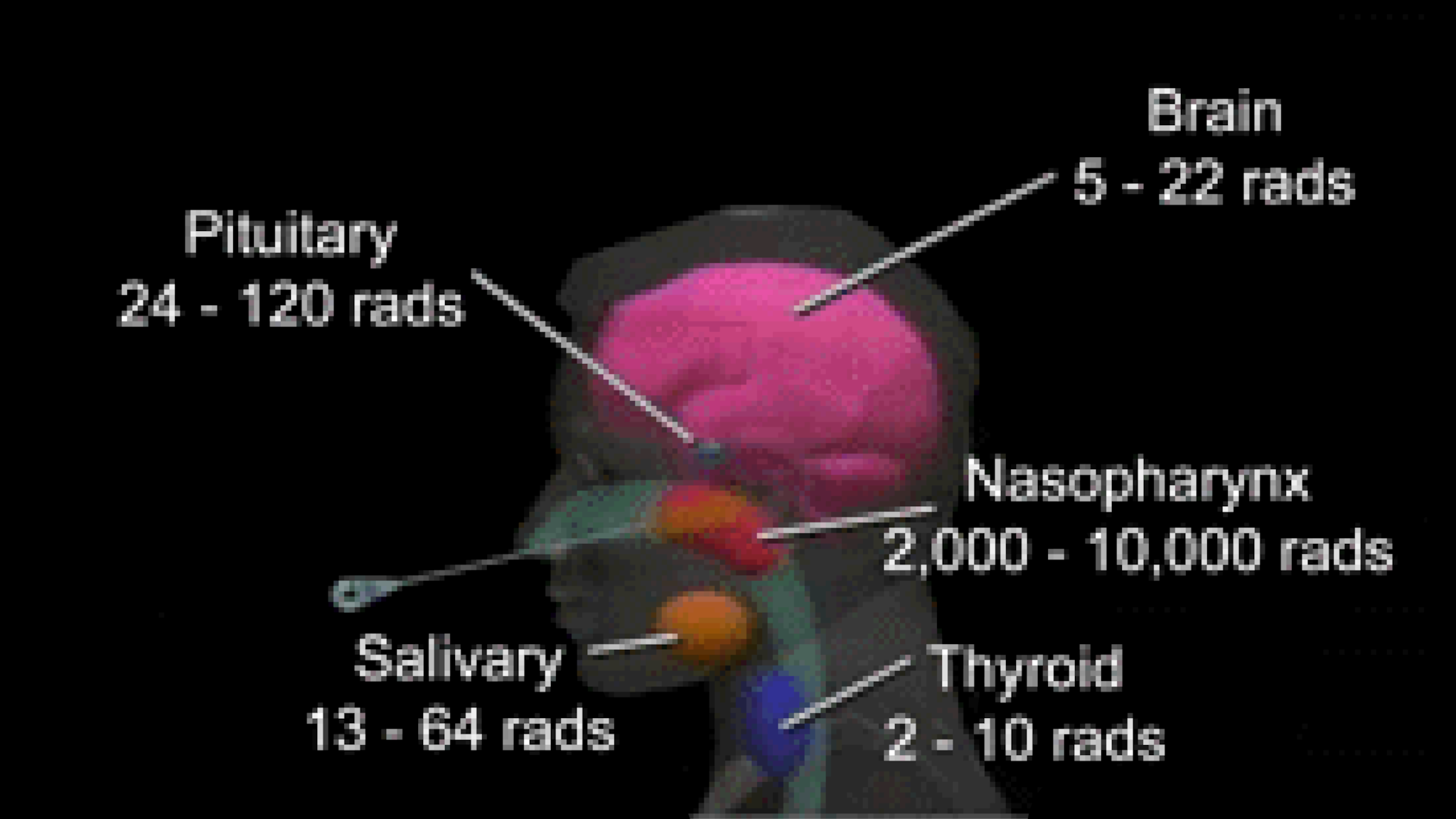
Estimates of Doses
- 2,000–10,000 rads to the mucosal lining of the nasopharynx
- 24–120 rads to the pituitary gland
- 13–64 rads to the salivary gland
- 5–22 rads to the brain
- 2–10 rads to the thyroid
Most of the radiation from nasopharyngeal radium was in the form of beta particles. The highest dose was typically delivered to the soft tissue of the nasopharynx. However, the background rate of cancer of the nasopharynx is low (0.6 per 100,000 persons). There is no documented evidence that the nasopharynx is as sensitive to radiation as thyroid or brain tissue.
Exposure scenario
If you do not recall the above situation, do you remember having adenoid and or hearing problems as a child? If so, you may want to ask a family member or your childhood doctor if they recall you receiving such a treatment.
Studies are inconclusive. However, because NRI may confer a modest increased risk, notify your doctor if you were treated with NRI. Your doctor may conduct a thorough head and neck examination at your next check-up.
Public Law 105-368 enacted in November 1998 makes the Department of Veterans Affairs' (VA) Ionizing Radiation program available to veterans who received radium treatments while they were in the military. Questions about this can be answered by a Veterans Benefits Counselor at local VA hospitals or the VA Regional Offices.
Where the data comes from
Study of military personnel
The Department of Veterans Affairs evaluated whether 1,214 NRI-exposed World War II submariners were at an increased risk of death compared to 3,176 untreated submariners (Kang et al, 2000). In this study, researchers found a small increased risk of death for the NRI-exposed veterans due to cancers, including cancers of the head and neck. However, these findings were not statistically significant.
Epidemiologic studies of health effects
Maryland study
A cohort study of 904 exposed and 2,021 unexposed persons during 1943-1960 (conducted by Sandler et al. in Maryland in 1982) showed a slight increased risk of head and neck cancers among exposed persons, but this was not statistically significant.
A follow-up study of this cohort was conducted in 2001 (Yeh et al, 2001). In this study, researchers found an elevated but statistically non-significant risk of developing certain cancers (brain, thyroid). However, they also found that the rates for other types of cancers (breast, endometrium, ovary, and prostate) were lower in the exposed population than in the non-exposed population. None of these findings were statistically significant.
Netherlands study
A cohort study of 2,510 exposed and 2,199 unexposed persons (conducted by Verduijn et al. in the Netherlands) did not document a statistically significant increase in head and neck cancers in the exposed group.
Follow-up investigators assessed whether cancer mortality of the Netherlands cohort was higher among 5,358 NRI-exposed individuals compared to 5,265 non-exposed patients (Ronckers et al, 2001). At the time of the study, they had been followed for an average of 31.6 years. The investigators found no increased risk of death from cancers of the head and neck, nor from brain tumors. They did, however, find evidence of a marginally statistically significant increase in death from non-Hodgkin lymphoma. They concluded that their study did not indicate that NRI-exposure in childhood was associated with an increased risk of cancer mortality.
In an analysis of the cancer incidence among 4,339 NRI-treated Dutch patients in the same Netherlands cohort (Ronckers et al, 2002b), the investigators found no elevated risk of cancer in general, nor of tumors of the head and neck in particular, compared to the 4,109 untreated participants.
The same researchers (Ronckers et al, 2002a) evaluated the occurrence of nonmelanoma skin cancer, benign tumors, and hormonal disorders in the same Dutch cohort. They found that the exposed population (3,440 patients) was not at increased risk of thyroid disorders or benign head and neck tumors, including pituitary adenomas and salivary gland tumors. However, they did find a marginally statistically significant increased risk of infertility in exposed men compared to the unexposed men.
Conclusions
Current studies do not indicate substantial increases in risks for neoplastic or other disease among those who received NRI treatments. Although these studies identify possible associations between NRI treatment and health effects, the findings are not consistent and thus no clear link between NRI exposure and cancer risk has been established.
CDC recommendations
Because the diseases that could be associated with this treatment are rare and the treatment may confer a modest additional risk of those diseases, CDC does not recommend screening for all patients who received the treatment. However, physicians may consider performing thorough head and neck examinations of patients with a history of NRI treatments. In addition, physicians who provide care for patients born before 1960 with head and neck complaints should ask the patients whether they have a history of NRI or other head and neck radiation treatments. Persons who recall being treated or believe they were treated with NRI should inform their physicians of the exposure. Some patients who received this treatment will be worried about it, and need the reassurance that is offered by a thorough and caring examination.
- Kang et al, 2000
- Sandler et al. in Maryland in 1982
- Yeh et al, 2001
- Verduijn et al. in the Netherlands
- Ronckers et al, 2001
- Ronckers et al, 2002b
- Ronckers et al, 2002a