
Study Syllabus for Classification of Radiographs of Pneumoconioses
Pathology Overview
Pathology Basis of Occupational Lung Disease
Asbestosis
Asbestos-Induced Benign Pleural Disease
Asbestos has a predilection for pleural injury, although the precise pathogenetic mechanisms by which fibers are deposited in the pleura and induce pleural changes are unclear [Oury 2004]. The nonneoplastic pleural disorders ascribed to asbestos include benign pleural effusion, plaques, and diffuse pleural fibrosis. Unexplained pleural effusions due to asbestos occur and may precede subsequent asbestos-related pleural disease. The histological changes in the pleura associated with asbestos-induced effusion have not been extensively documented, but chronic pleuritis with organizing fibrin may be seen. The pleural fluid is exudative and either serous or serosanguineous with leukocytosis. The diagnosis of asbestos-related pleural effusion is one of exclusion and requires extended follow-up to rule out malignancy. Chronic effusions may lead to diffuse pleural fibrosis [Gaensler and Kaplan 1971; McCloud et al. 1985].
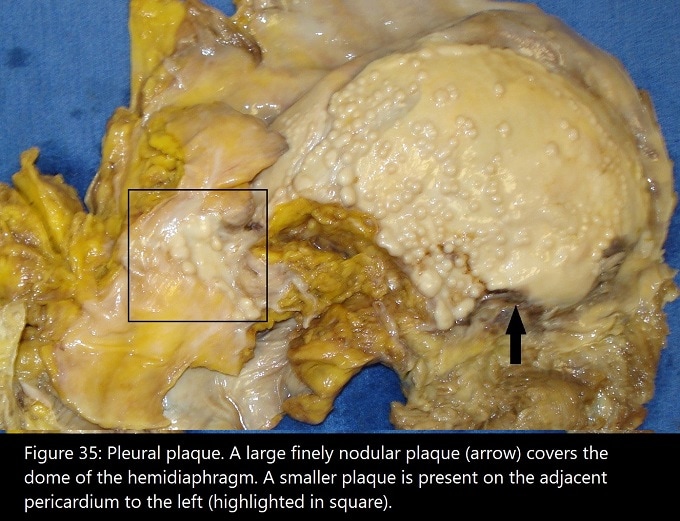
Pleural plaques constitute an important marker of asbestos exposure. Plaques are defined as discrete, elevated, circumscribed fibrotic lesions usually located on the parietal pleura [Oury 2004]. Macroscopically, plaques are pearly white, rubbery, or hard because of calcification, with scalloped edges. The shape varies from flat and discoid to nodular, and the distribution frequently parallels the spine, with extension along the ribs. Diaphragmatic plaques are usually concentrated in the area of the central tendon (Fig. 35). Histologically, plaques are composed of coarse eosinophilic bundles of acellular collagen having a basket-weave pattern (Fig. 36). A variable degree of basophilic calcification is often present. Asbestos bodies are rarely identified histologically in plaques.
{kind=link}
Diffuse pleural fibrosis, as opposed to pleural plaque, represents fibrous thickening of the parietal and/or visceral pleura often associated with dense pleural adhesions [McCloud et al. 1985]. The extent of fibrosis varies from minimal involvement to complete circumscription of the lung by a rind of thick fibrous tissue, resembling the gross appearance of malignant mesothelioma. Histologically, diffuse pleural fibrosis consists of coarse collagen bundles in a basket-weave pattern with focal calcification, resembling the histology of pleural plaques [Churg 1998a; Roggli et al. 2010; Oury 2004; Stephens et al. 1987] (Fig. 37). An associated lesion occasionally seen in the lung beneath areas of diffuse pleural fibrosis or adherent pleural plaques is rounded atelectasis [Oury 2004; Hillerdal 1989; “Case records,” 1983] (Fig. 38). The pathogenesis of rounded atelectasis is thought to represent pleural infolding in conjunction with organizing pleuritis or pleural effusion (Fig. 39). As a consequence of organization and fibrosis of the visceral pleural surface, the infolded pleura and surrounding atelectatic lung become irreversibly fixed in position. Macroscopically, the subpleural parenchyma is vaguely nodular, with a spongy texture surrounding a linear retraction of fibrotic visceral pleura. Histologically, compressed fibrotic alveolar parenchyma is oriented around a deep pleural fold, which can be highlighted with tissue elastic stains (Fig. 39). Although asbestos is considered to be the major cause, virtually any cause of pleural fibrosis can result in rounded atelectasis [Hillerdal 1989].