Residents Living in Residential Care Facilities: United States, 2010
- Key findings
- In 2010, the majority of residents were non-Hispanic white, female, and aged 85 and over.
- Nearly 2 in 10 residents were Medicaid beneficiaries.
- Almost 4 in 10 residents received assistance with three or more activities of daily living.
- Almost three-fourths of residents had ever been diagnosed with at least 2 of the 10 most common chronic conditions.
- Summary
- Definitions
- Data sources and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 91, April 2012
PDF Version (500 KB)
Christine Caffrey, Ph.D.; Manisha Sengupta, Ph.D.; Eunice Park-Lee, Ph.D.; Abigail Moss; Emily Rosenoff, M.P.A.; and Lauren Harris-Kojetin, Ph.D.
Key findings
Data from the 2010 National Survey of Residential Care Facilities
- The majority of residents living in residential care facilities in 2010 were non-Hispanic white and female. More than one-half of all residents were aged 85 and over.
- Nearly 2 in 10 residents were Medicaid beneficiaries, and almost 6 in 10 residents under age 65 had Medicaid.
- Almost 4 in 10 residents received assistance with three or more activities of daily living, of which bathing and dressing were the most common.
- More than three-fourths of residents have had at least 2 of the 10 most common chronic conditions; high blood pressure and Alzheimer’s disease and other dementias were the most prevalent.
Persons living in state-regulated residential care facilities (RCFs)—such as residents of assisted living communities—receive housing and supportive services because they cannot live independently but generally do not require the skilled level of care provided by nursing homes. The ability to provide a comprehensive picture of the long-term care industry has been hampered by a lack of data on RCFs (1–4). Previous estimates of the number of residents in RCFs vary depending on how RCFs are defined (5–7). A recent NCHS data brief (5) reported that for each day in 2010, 733,300 persons were residents of RCFs nationwide. Using data from the first nationally representative survey of RCFs with four or more beds, this report presents national estimates of these RCF residents by selected resident characteristics.
Keywords: assisted living, long-term care
In 2010, the majority of residents were non-Hispanic white, female, and aged 85 and over.
- Nine in ten residents were non-Hispanic white (91%), and seven in ten residents were female (70%) (Figure 1).
- More than one-half of residents were aged 85 and over (54%), and more than one-quarter of residents were aged 75–84 (27%). The remaining one-fifth of residents were about evenly split between those aged 65–74 (9%) and those under age 65 (11%).
- The median length of stay among all current residents at the time of interview was 671 days, or about 22 months (data not shown).
Figure 1. Selected characteristics of residential care residents: United States, 2010
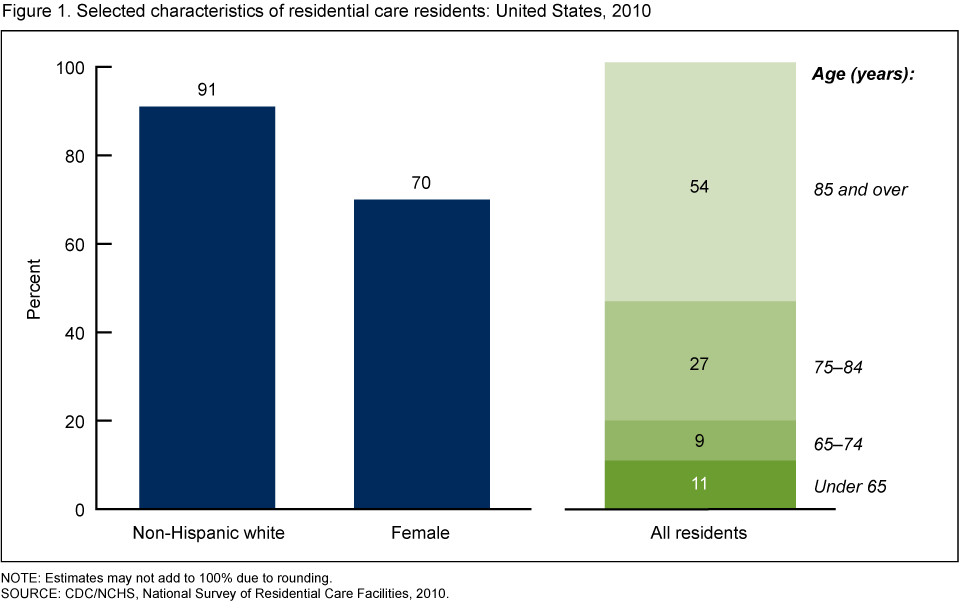
NOTE: Estimates may not add to 100% due to rounding.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
Nearly 2 in 10 residents were Medicaid beneficiaries.
- Medicaid paid for at least some of the RCF services for 19% of residents (Figure 2).
- Younger residents were more likely to have Medicaid than older residents. Almost 6 in 10 residents under age 65 had Medicaid (56%) compared with 39% of residents aged 65–74, 16% of residents aged 75–84, and 10% of residents aged 85 and over.
- In 2010, the mean national total monthly charge per resident for residential care was $3,165 (data not shown).
Figure 2. Residential care residents with Medicaid, by age: United States, 2010
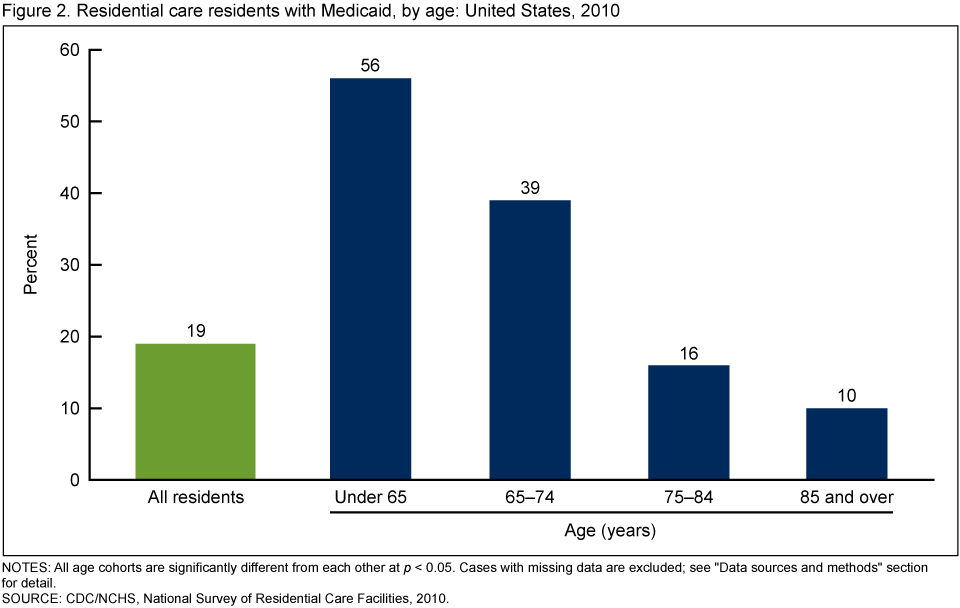
NOTES: All age cohorts are significantly different from each other at p < 0.05. Cases with missing data are excluded; see “Data sources and methods” section for detail.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
Almost 4 in 10 residents received assistance with three or more activities of daily living.
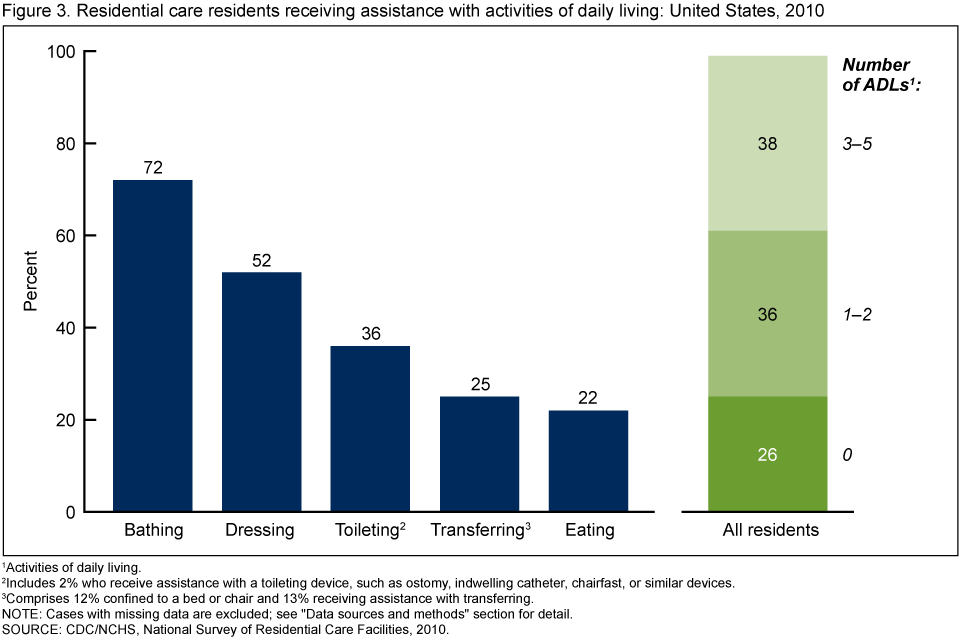
- About three-quarters of all residents received assistance with bathing (72%), over one-half received assistance with dressing (52%), more than one-third received assistance with toileting (36%), one-quarter received assistance with transferring (25%), and more than one-fifth received assistance with eating (22%) (Figure 3).
- Thirty-eight percent of RCF residents received assistance with three or more of these activities of daily living (ADLs), an additional 36% received assistance with one or two of the ADLs, and 26% did not receive assistance with any ADL
Figure 3. Residential care residents receiving assistance with activities of daily living: United States, 2010
1Activities of daily living.
2Includes 2% who receive assistance with a toileting device, such as ostomy, indwelling catheter, chairfast, or similar devices.
3Comprises 12% confined to a bed or chair and 13% receiving assistance with transferring.
NOTE: Cases with missing data are excluded; see “Data sources and methods” section for detail.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
Almost three-fourths of residents had ever been diagnosed with at least 2 of the 10 most common chronic conditions.
- The 10 most common chronic conditions among residents were high blood pressure (57%), Alzheimer’s disease or other dementias (42%), heart disease (34%), depression (28%), arthritis (27%), osteoporosis (21%), diabetes (17%), chronic obstructive pulmonary disease and allied conditions (15%), cancer (11%), and stroke (11%) (Figure 4).
- More than one-quarter of RCF residents had ever been diagnosed with 4–10 of the most common chronic conditions (26%); one-half of residents had ever been diagnosed with 2–3 of the most common chronic conditions; 18% had ever been diagnosed with one of these chronic conditions; and the remaining 6% had never been diagnosed with these conditions (Figure 4).
Figure 4. Most common chronic conditions of residential care residents: United States, 2010
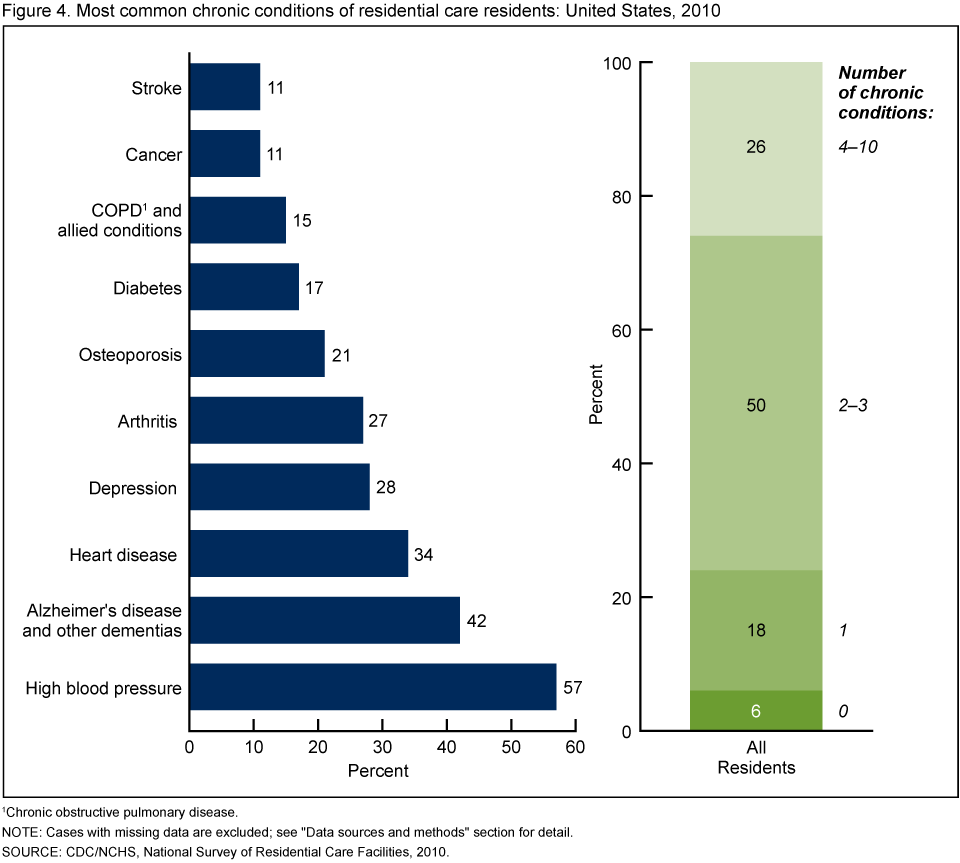
1Chronic obstructive pulmonary disease.
NOTE: Cases with missing data are excluded; see “Data sources and methods” section for detail.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
Summary
In 2010, residential care residents were mostly female, non-Hispanic white, and aged 85 and over, and had a median length of stay of about 22 months. For about 20% of residents—or 137,700 persons—Medicaid paid for at least some long-term care services provided by the RCF. This estimate is similar to that found in a recent study (3). Almost 40% of all residential care residents received assistance with three or more ADL limitations, and over 40% had Alzheimer’s disease or other dementias. These findings suggest a vulnerable population with a high burden of functional and cognitive impairment.
Residential care is an important component of the U.S. long-term care system. This report presents national estimates of people living in RCFs, using data from the first-ever national probability sample survey of RCFs with four or more beds. This brief profile of residential care residents may provide useful information to policymakers, providers, and consumer advocates as they plan for the future long-term care needs of older as well as younger adults. In addition, these findings serve as baseline national estimates as researchers continue to track the growth of and changes in the residential care industry.
Definitions
Length of stay: Derived from the month and year in which the resident first moved into the RCF and the month and year of the interview.
Medicaid beneficiary: A resident who, during the 30 days before the interview, had any of his or her long-term care services at the RCF paid by Medicaid.
Charges: The total charge for the month prior to the interview, including the basic monthly charge and any charges for additional services.
Assistance with activities of daily living (ADLs): Refers to receiving any assistance in the five ADLs (bathing, dressing, transferring, using the toilet, and eating) that reflect a resident’s capacity for self-care. A summary variable was created with three categories: no limitations, 1–2 limitations, and 3–5 limitations. For residents confined to a bed or chair, the question about whether the resident received assistance with transferring was not asked in the survey. For the current analyses, the 12% of residents chair-ridden or bedridden were defined as receiving assistance in the transferring and summary ADL variables. The 2% of residents who receive assistance with a device to use the toilet, such as an ostomy, catheter, or chairfast device, were defined as receiving assistance in the toileting and summary ADL variables.
Most common chronic conditions: Includes the 10 most common chronic conditions that residents were ever diagnosed as having by a doctor or other health professional, based on the RCF staff respondent’s reference to the resident’s medical record or personal knowledge of the resident. A summary variable was created with four categories: no conditions, one condition, 2–3 conditions, and 4–10 conditions.
Data sources and methods
Resident data from the 2010 National Survey of Residential Care Facilities (NSRCF) were used for these analyses. To be eligible for NSRCF, RCFs must be licensed, registered, listed, certified, or otherwise regulated by the state; have four or more licensed, certified, or registered beds; and provide room and board with at least two meals a day, around-the-clock on-site supervision, and help with personal care such as bathing and dressing or health-related services such as medication management. These RCFs also serve a predominantly adult population. RCFs licensed to exclusively serve the mentally ill or developmentally disabled populations were excluded. Nursing homes also were excluded unless they had a unit or wing meeting the above definition and their residents could be separately enumerated.
The 2010 NSRCF used a stratified two-stage probability sample design. The first stage was the selection of RCFs from the sampling frame representing the universe of RCFs. For the 2010 NSRCF, 3,605 RCFs were sampled with probability proportional to facility size. Interviews were completed with 2,302 RCFs, for a first-stage, facility-level weighted response rate of 81%, which was weighted for differential probabilities of selection. In the second stage of sampling, 3–6 current residents were selected depending on RCF bed size. All data collected on sampled residents came from interviews with RCF staff who answered questions by referring to the residents’ records or their own knowledge of the residents; residents were never interviewed. The second-stage, resident-level weighted response rate was 99%. A detailed description of NSRCF sampling design, data collection, and procedures is provided both in a previous report (8) and on the NSRCF website.
Differences among subgroups were evaluated using chi-square and t tests. If chi-square tests were statistically significant, a post hoc t-test procedure was used to make pairwise comparisons. Significant results from the post hoc procedure are reported here. All significance tests were two-sided using p < 0.05 as the level of significance. The difference between any two estimates is reported only if it is statistically significant. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not statistically significant. Data analyses were performed using the statistical package SAS-callable SUDAAN version 10.0 (9). Cases with missing data were excluded from the analyses on a variable-by-variable basis. The percentage of weighted cases with missing data varied between 0.01% and 2.5%. Because estimates were rounded, individual estimates may not sum to totals.
About the authors
Christine Caffrey, Manisha Sengupta, Eunice Park-Lee, Abigail Moss, and Lauren Harris-Kojetin are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Care Statistics. Emily Rosenoff is with the Department of Health and Human Services, Assistant Secretary for Planning and Evaluation’s Office of Disability, Aging, and Long-Term Care Policy.
References
- Spillman BC, Black KJ. The size of the long-term care population in residential care: A review of estimates and methodology. Prepared for U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy. Washington, DC: The Urban Institute. 2005.
- Spillman BC, Black KJ. The size and characteristics of the residential care population: Evidence from three national surveys. Prepared for U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy. Washington, DC: The Urban Institute. 2006.
- Polzer K. Assisted living state regulatory review 2011. Washington, DC: National Center for Assisted Living. 2011.
- MetLife Mature Market Institute. Market Survey of Long-Term Care Costs. Westport, CT. 2010.
- Park-Lee E, Caffrey C, Sengupta M, et al. Residential care facilities: A key sector in the spectrum of long-term care providers in the United States. NCHS data brief, no 78. Hyattsville, MD: National Center for Health Statistics. 2011.
- Mollica R, Sims-Kastelein K, O’Keeffe J. Residential care and assisted living compendium: 2007. Prepared for U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy. Washington, DC: RTI International. 2007.
- Stevenson DG, Grabowski DC. Sizing up the market for assisted living. Health Aff 29(1): 35–43. 2010.
- Moss AJ, Harris-Kojetin LD, Sengupta M, et al. Design and operation of the 2010 National Survey of Residential Care Facilities. National Center for Health Statistics. Vital Health Stat 1(54). 2011.
- SUDAAN, release 10.0 [computer software]. Research Triangle Park, NC: RTI International. 2008.
Suggested citation
Caffrey C, Sengupta M, Park-Lee E, et al. Residents living in residential care facilities: United States, 2010. NCHS data brief, no 91. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director