Health Care Access and Utilization Among Adults Aged 18–64, by Poverty Level: United States, 2013–2015
- Key findings
- The percentage of uninsured adults decreased from 2013 through 2015 for all poverty level subgroups.
- The percentage of poor and near-poor adults with a usual place to go for medical care increased from 2013 through 2015.
- The percentage of poor and near-poor adults who had seen or talked to a health professional in the past 12 months increased from 2013 through 2015.
- The percentage of adults aged 18–64 who did not obtain needed medical care due to cost decreased from 2013 through 2015 for all poverty level subgroups.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 262, October 2016
PDF Version (305 KB)
Michael E. Martinez, M.P.H., M.H.S.A. and Brian W. Ward, Ph.D.
Key findings
Data from the National Health Interview Survey, 2013–2015
- From 2013 through 2015, the percentage of adults aged 18–64 who were uninsured at the time of interview decreased for poor (40.0% to 26.2%), near-poor (37.8% to 23.9%), and not-poor (11.7% to 7.7%) adults.
- The percentage of adults aged 18–64 who had a usual place to go for medical care increased for poor (66.9% to 73.6%) and near-poor (71.1% to 75.9%) adults.
- The percentage of adults aged 18–64 who had seen or talked to a health professional in the past 12 months increased for poor (73.2% to 75.8%) and near-poor (71.9% to 75.9%) adults.
- The percentage of adults aged 18–64 who did not obtain needed medical care due to cost at some time during the past 12 months decreased for poor (16.8% to 12.4%), near-poor (14.6% to 11.0%), and not-poor (4.9% to 3.8%) adults.
In 2014, U.S. adults could purchase a private health insurance plan through the Health Insurance Marketplace or state-based exchanges established as part of the Affordable Care Act (ACA). Additionally, under ACA some states opted to expand Medicaid coverage to low-income adults. Individuals living in or near poverty may have benefited disproportionately from these changes given their lower rates of health insurance coverage (1). Data from the 2013–2015 National Health Interview Survey (NHIS) are used to describe recent changes in health insurance coverage and selected measures of health care access and utilization for adults aged 18–64 by family poverty level.
Keywords: Affordable Care Act, medical care, health insurance, National Health Interview Survey
The percentage of uninsured adults decreased from 2013 through 2015 for all poverty level subgroups.
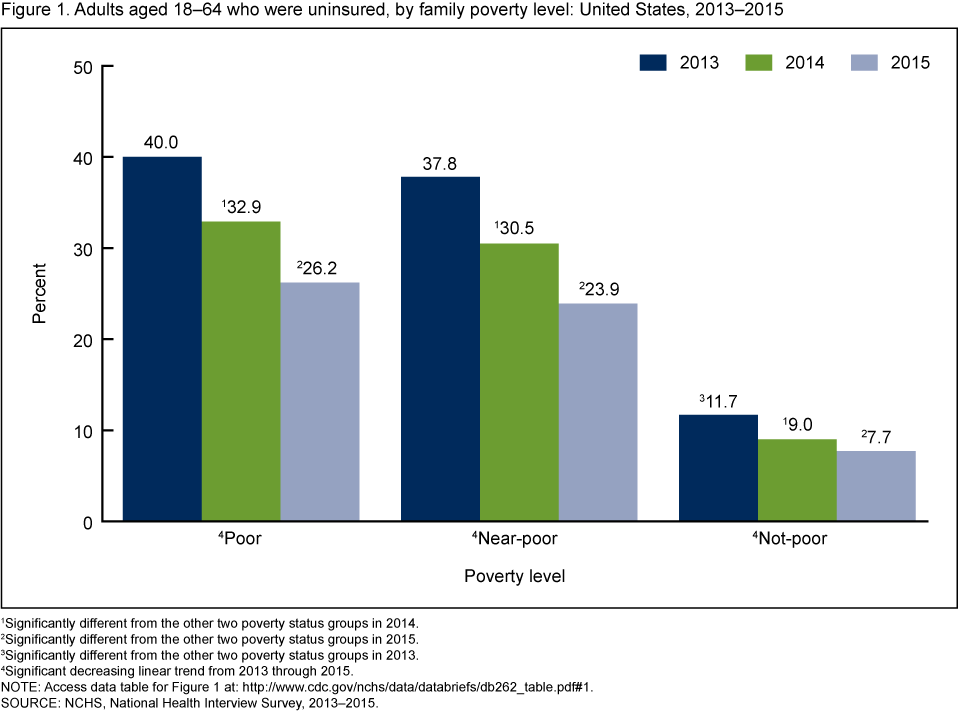
- From 2013 through 2015, the percentage of adults aged 18–64 who were uninsured at the time of interview decreased for poor (from 40.0% to 26.2%), near-poor (from 37.8% to 23.9%), and not-poor (from 11.7% to 7.7%) adults (Figure 1).
- From 2013 through 2015, not-poor adults aged 18–64 were the least likely to be uninsured.
Figure 1. Adults aged 18–64 who were uninsured, by family poverty level: United States, 2013–2015
1Significantly different from the other two poverty status groups in 2014.
2Significantly different from the other two poverty status groups in 2015.
3Significantly different from the other two poverty status groups in 2013.
4Significant decreasing linear trend from 2013 through 2015.
NOTE: Access data table for Figure 1.
SOURCE: NCHS, National Health Interview Survey, 2013–2015.
The percentage of poor and near-poor adults with a usual place to go for medical care increased from 2013 through 2015.
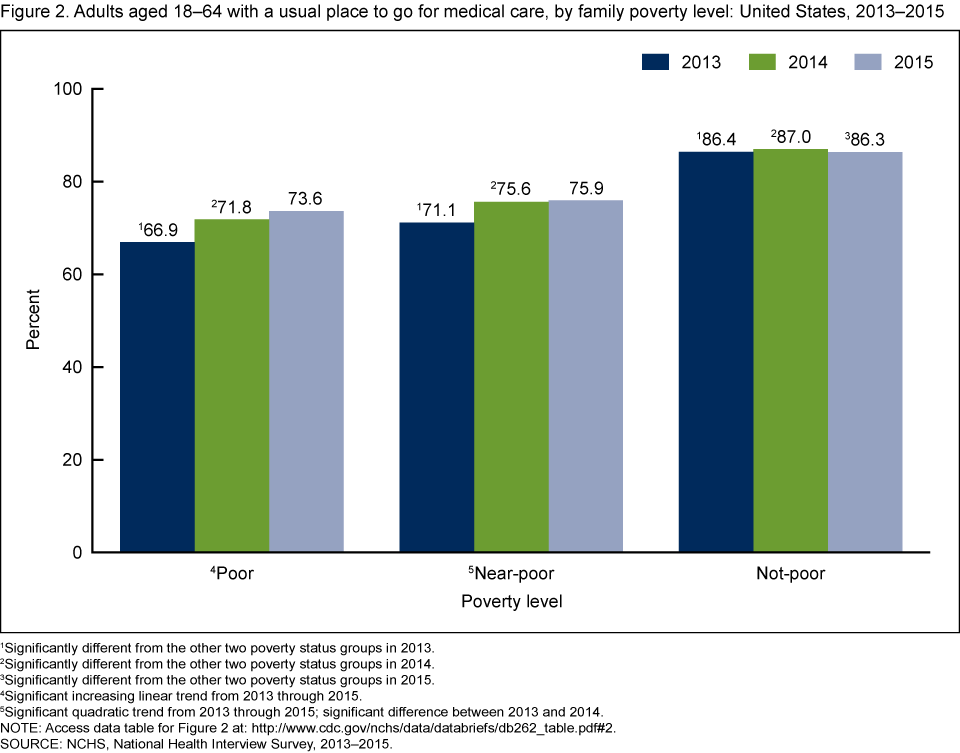
- From 2013 through 2015, the percentage of adults aged 18–64 who had a usual place to go for medical care increased from 66.9% to 73.6% for poor adults, and from 71.1% to 75.9% for near-poor adults (Figure 2).
- There was an increasing linear trend in the percentage of poor adults aged 18–64 who had a usual place to go for medical care from 2013 through 2015, but for near-poor adults, there was an increase from 2013 through 2014 with no significant change from 2014 through 2015.
- From 2013 through 2015, the percentage of not-poor adults aged 18–64 who had a usual place to go for medical care did not change significantly.
- From 2013 through 2015, not-poor adults aged 18–64 were the most likely to have a usual place to go for medical care.
Figure 2. Adults aged 18–64 with a usual place to go for medical care, by family poverty level: United States, 2013–2015
1Significantly different from the other two poverty status groups in 2013.
2Significantly different from the other two poverty status groups in 2014.
3Significantly different from the other two poverty status groups in 2015.
4Significant increasing linear trend from 2013 through 2015.
5Significant quadratic trend from 2013 through 2015; significant difference between 2013 and 2014.
NOTE: Access data table for Figure 2.
SOURCE: NCHS, National Health Interview Survey, 2013–2015.
The percentage of poor and near-poor adults who had seen or talked to a health professional in the past 12 months increased from 2013 through 2015.
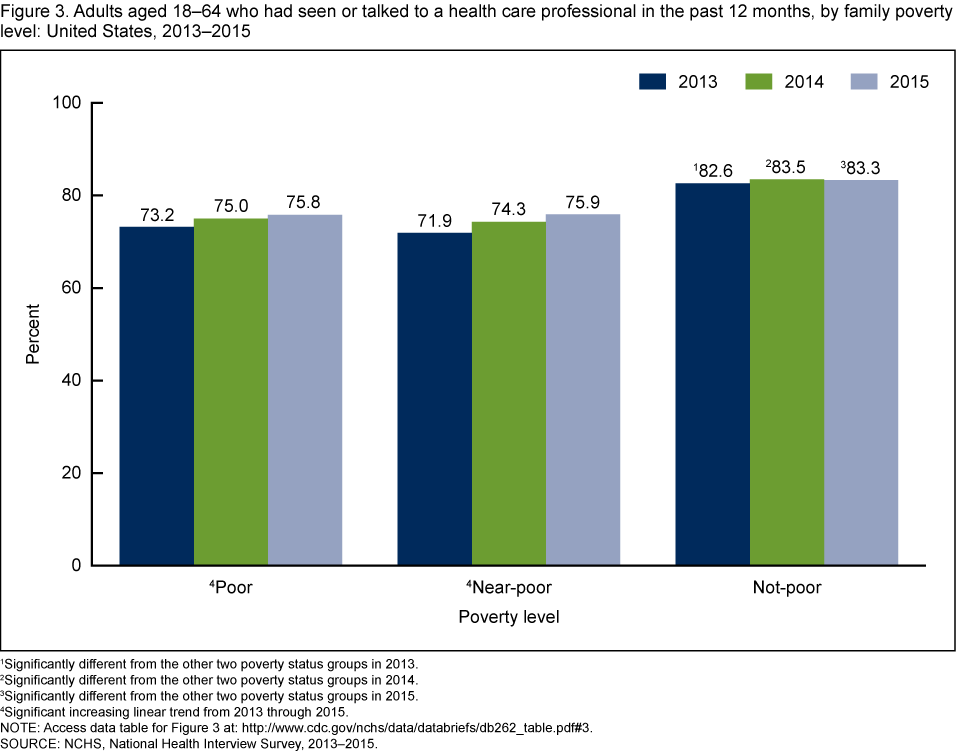
- From 2013 through 2015, the percentage of adults aged 18–64 who had seen or talked to a health professional in the past 12 months increased from 73.2% to 75.8% for poor adults, and from 71.9% to 75.9% for near-poor adults (Figure 3).
- From 2013 through 2015, the percentage of not-poor adults aged 18–64 who had seen or talked to a health professional in the past 12 months did not change significantly.
- From 2013 through 2015, not-poor adults aged 18–64 were the most likely to have seen or talked to a health professional in the past 12 months.
Figure 3. Adults aged 18–64 who had seen or talked to a health care professional in the past 12 months, by family poverty level: United States, 2013–2015
1Significantly different from the other two poverty status groups in 2013.
2Significantly different from the other two poverty status groups in 2014.
3Significantly different from the other two poverty status groups in 2015.
4Significant increasing linear trend from 2013 through 2015.
NOTE: Access data table for Figure 3.
SOURCE: NCHS, National Health Interview Survey, 2013–2015.
The percentage of adults aged 18–64 who did not obtain needed medical care due to cost decreased from 2013 through 2015 for all poverty level subgroups.
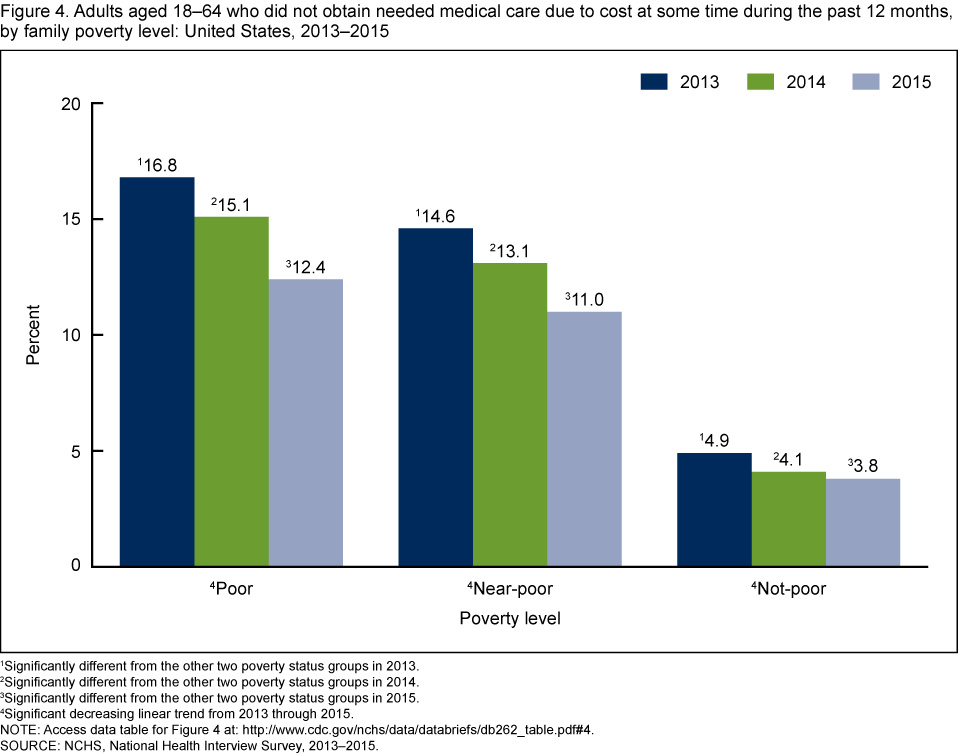
- From 2013 through 2015, the percentage of adults aged 18–64 who did not obtain needed medical care due to cost at some time during the past 12 months decreased for poor (from 16.8% to 12.4%), near-poor (from 14.6% to 11.0%), and not-poor (from 4.9% to 3.8%) adults (Figure 4).
- From 2013 through 2015, poor adults aged 18–64 were the most likely to not obtain needed medical care due to cost at some time during the past 12 months.
- From 2013 through 2015, not-poor adults aged 18–64 were the least likely to not obtain needed medical care due to cost at some time during the past 12 months.
Figure 4. Adults aged 18–64 who did not obtain needed medical care due to cost at some time during the past 12 months, by family poverty level: United States, 2013–2015
1Significantly different from the other two poverty status groups in 2013.
2Significantly different from the other two poverty status groups in 2014.
3Significantly different from the other two poverty status groups in 2015.
4Significant decreasing linear trend from 2013 through 2015.
NOTE: Access data table for Figure 4.
SOURCE: NCHS, National Health Interview Survey, 2013–2015.
Summary
For all family poverty level groups examined, significant decreases were observed from 2013 through 2015 in the percent uninsured. Insurance can lead to improvements in health care access and utilization. Indeed, relative to 2013, poor and near-poor adults aged 18–64 in 2015 were significantly more likely to have a usual place for medical care, and, within the past 12 months, they were more likely to have seen or talked to a health professional. However, for not-poor adults aged 18–64, there was no statistically significant change in having a usual place for medical care and having seen or talked to a health professional within the past 12 months. All family poverty level groups examined did show significant decreases from 2013 through 2015 for those who did not obtain needed medical care due to cost at some time during the past 12 months.
Despite improvements in insurance coverage and health care access for poor and near-poor adults aged 18–64, they were still less likely than not-poor adults to have a usual place for medical care and to have seen or talked to a health care professional in the past 12 months.
Definitions
Did not obtain needed medical care due to cost in the past 12 months: Based on the question, “During the past 12 months, was there any time when [person] needed medical care, but did not get it because [person] couldn’t afford it?” Responses exclude dental care.
Federal poverty level: Determined by dividing the total family income by the U.S. Census Bureau’s poverty threshold specific to a family’s size and age of the members in that family. This ratio is multiplied by 100, and family poverty level was determined based on where a family fell relative to certain thresholds. Adults were considered poor if their family poverty level fell below 100% of the threshold. Adults were considered near-poor if their family poverty level fell at or above 100% but less than 200%. And adults were considered not-poor if their family poverty level fell at or above 200%.
Seen or talked to a health professional in the past 12 months: Based on combined responses of “6 months or less” and “more than 6 months, but not more than 1 year ago” to the survey question, “About how long has it been since you last saw or talked to a doctor or other health care professional about your own health? Include doctors seen while a patient in a hospital.”
Uninsured: Determined by not having any private health insurance, Medicare, Medicaid, CHIP (Children’s Health Insurance Program), state-sponsored or other government-sponsored health plan, or military plan at the time of interview. A person was also defined as uninsured if he or she had only Indian Health Service coverage or had only a private plan that paid for one type of service, such as accidents or dental care. The analyses excluded persons with unknown health insurance status (about 1% of respondents each year).
Usual place to go for medical care: Based on the question, “Is there a place that you usually go to when you are sick or need advice about your health?” If there was at least one such place, then a follow-up question was asked: “What kind of place [is it/do you go to most often]—a clinic, doctor’s office, emergency room, or some other place?” Adults who indicated that the emergency room was their usual place for care were considered not to have a usual place for health care.
Data source and methods
Data from the 2013–2015 NHIS were used for this analysis. NHIS is a multipurpose health survey conducted continuously throughout the year by the National Center for Health Statistics (NCHS). Interviews are conducted in person in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. Questions about health insurance coverage and not obtaining needed medical care are from the survey’s Family Core component, while questions about a usual place to go for medical care and having seen or talked to a health professional in the past 12 months are from the Sample Adult component. The Family Core component collects information on all family members, and the Sample Adult component collects additional data from one randomly selected adult (the “sample adult”). NHIS-imputed income files were used to help create the poverty variables. For further information about NHIS, including the questionnaire, visit the NHIS website.
All analyses used weights to produce national estimates. Data weighting procedures are described elsewhere (2). Point estimates and their estimated variances were calculated using SUDAAN software (3) and the Taylor series linearization method to account for the complex design of NHIS. Two-sided significance tests at the 0.05 level were used to compare estimates. All estimates shown in this report meet the NCHS standard of reliability (relative standard error less than or equal to 30%). Logistic regression was used to assess trends.
About the authors
Michael E. Martinez and Brian W. Ward are with the National Center for Health Statistics, Division of Health Interview Statistics.
References
- Cohen RA, Martinez ME, Zammitti EP. Health insurance coverage: Early release of estimates from the National Health Interview Survey, January–March 2016. National Center for Health Statistics. September 2016.
- Parsons VL, Moriarity C, Jonas K, et al. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
- RTI International. SUDAAN (Release 11.0.0) [computer software]. 2012.
Suggested citation
Martinez ME, Ward BW. Health care access and utilization among adults aged 18–64, by poverty level: United States, 2013–2015. NCHS data brief, no 262. Hyattsville, MD: National Center for Health Statistics. 2016.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Interview Statistics
Marcie L. Cynamon, Director
Stephen J. Blumberg, Ph.D., Associate Director for Science