Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Data Sources
Implementation of Laboratory Order Data in BioSense Early
Event Detection and Situation Awareness System
Haobo Ma,1 H. Rolka,1 K. Mandl,2 D.
Buckeridge,3,4 A. Fleischauer,1 J. Pavlin5
1CDC, Atlanta, Georgia;
2Children's Hospital Boston, Boston, Massachusetts and Harvard Medical School, Boston, Massachusetts; 3Palo Alto Veterans Health Care, Palo Alto, California; 4Stanford University, Stanford, California;
5Walter Reed Army Institute of Research, Silver Spring, Maryland
Corresponding author: Haobo Ma, CDC, 1600 Clifton Rd., NE, MS
E-06, Atlanta, GA 30333, Telephone: 404-498-6283; Fax: 404-498-3225; Email: HMa@cdc.gov.
Disclosure of relationship: The contributors of this report have disclosed that they have no financial interest, relationship, affiliation, or other association with any organization that might represent a conflict of interest. In addition, this report does not contain any discussion
of unlabeled use of commercial products or products for investigational use.
Abstract
Introduction: Laboratory test orders constitute an early outbreak data source. CDC receives laboratory
order data in HL7 format from the Laboratory Corporation of America (LabCorp) and plans to use the data in the BioSense Early
Event Detection and Situation Awareness System.
Methods: These LabCorp data contain information on tests ordered and include the type of test ordered and
the International Classification of Diseases, Ninth Revision, Clinical Modification
(ICD-9-CM)-coded reasons for the order. A consensus panel was formed to group test orders on the basis of expert opinion into eight standard syndrome categories to provide an additional data source for early outbreak detection. A laboratory order taxonomy was
developed and used in the mapping consolidation phase. The five main classes of this taxonomy are miscellaneous functional tests, fluid screening tests, system-specific tests, tests for specific infections (by
primary manifestation), and tests for specific noninfectious diseases.
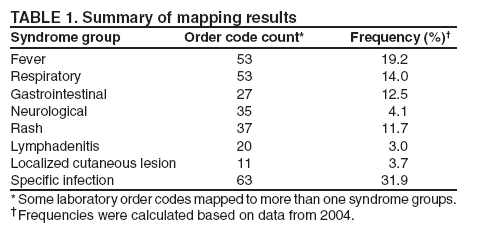
Results: Summary of numbers of laboratory order codes in each syndrome category are fever (53),
respiratory (53), gastrointestinal (27), neurological (35), rash (37), lymphadenitis (20), localized cutaneous lesion (11), and specific infection (63).
Conclusion: With the daily use of laboratory order data in BioSense, the actual distribution of laboratory order codes
in syndrome groups can be evaluated, allowing modification of the mapping.
Introduction
Laboratory test orders constitute an early outbreak data source because test ordering occurs earlier in patients' health service than laboratory test results or final diagnoses. Three basis exists for using laboratory order data for early outbreak detection. First, laboratory orders reflect the physician's
assessment of the patient's condition and intent to confirm or
differentiate diagnoses. Second, when laboratory order data feeds directly from national laboratories are used, it can provide good population coverage. Finally, laboratory orders in large hospitals or national laboratories are transmitted in the standard Health Level 7 (HL7) format electronically, which provides timely data collection and helps ensure data quality. Use of HL7
is increasingly important when constructing automated
early outbreak detection systems to handle large data volume. In
addition, standard laboratory terminology such as the Logical Observation Identifiers, Names, and Codes (LOINC) has been well adopted
for laboratory orders in commercial labs (1). Using LOINC codes in laboratory order data improves interoperability and scalability for the detection system.
CDC's BioSense program receives laboratory order data from LabCorp, which operates a nationwide network of 31 primary testing locations, and approximately 1,100 patient service centers. It tests more than 340,000 specimens daily
Methods
Laboratory Order Data
CDC receives a daily transmission of HL7 laboratory
orders from LabCorp. Data files are sent to CDC from LabCorp
using the Public Health Information Network Messaging System (PHINMS) with digital certificates and encryption. Immediately upon receipt, HL7 messages are mapped to XML
format and stored in a data warehouse.
The laboratory order data contain patient age, sex, ZIP code, timestamp information and LabCorp propriety codes and corresponding LOINC codes for each laboratory test ordered. Each laboratory message might have more than one
laboratory order placed in one patient encounter. Each laboratory order has one or more subcomponents. For example, a hepatitis B laboratory order will include various antibodies and antigens as its subcomponents. In addition, International Classification of Diseases, Ninth Revision, Clinical
Modification (ICD-9-CM) codes are used as reasons for laboratory orders. CDC BioSense does not receive laboratory order results associated with each order.
All data received are anonymous and cannot be traced back to the patient. Use of patient ZIP codes and year of birth are not sufficient for patient identification in the large population areas surveyed.
Consensus Panel
When the laboratory order data are identified, laboratory order codes are mapped into syndrome groups. The objective
for the mapping was to provide useful information for early event detection.
A consensus panel of 19 persons was organized with expertise in surveillance, infectious diseases, and medical informatics to perform the mapping. Participants included representatives from the Council of State and Territorial Epidemiologists,
the Department of Homeland Security, Harvard Medical School, the Johns Hopkins University Applied Physics Laboratory, Stanford Medical Informatics, the Walter Reed Army Institute of Research, the New York City Department of Hygiene and Mental Health, and CDC. The expertise of domain
experts was used to ensure the validity and reliability of the
mapping result.
Mapping Procedures
The 11 syndrome groups used in BioSense have been
defined by a multiagency working group. The
syndromes included fever, respiratory, gastrointestinal, lymphadenitis, specific infection,
localized cutaneous lesion, rash, neurologic, botulism-like, hemorrhagic illness, and severe illness or death potentially caused by infectious disease. Detailed syndrome definitions are available on the CDC Emergency Preparedness and Response website
(http://www.bt.cdc.gov/surveillance/syndromedef). For the laboratory test mapping, the working group determined that laboratory order codes for botulism-like illness, hemorrhagic illnesses, and severe illness or death do not exist; LabCorp data feeds and these syndromes were
not included in the mapping.
Domain experts determined the mapping, which was performed in stages. At each stage, a subset of the
panel worked on the mapping problem, and the rest of the panel reviewed the results and arrived at a consensus. Four group members
volunteered for the first round of mapping. They mapped each laboratory order to one or more syndromes using a simple mapping form. For example, a laboratory order with the name of influenza A and B antibodies, quantitative can be mapped to
respiratory syndrome group. After receiving the four sets of results, three panel members consolidated the results. During these processes, other panel members provided input and
advice.
The syndrome mapping of each laboratory order code was combined and represented as numbers. The number in combined results reflected the number of experts' selections in that syndrome group for a specific laboratory order code.
To reduce variations in the mapping results, the following constraints were enforced on the mapping:
Mapping results are consistent within the same LabCorp laboratory order panel or profile group.
Mapping results are consistent with LabCorp's online documentation of its use and specimen.
Laboratory order codes classified in the same disease or pathogen group in a laboratory order code
taxonomy are mapped in the same way.
Laboratory Order Code Taxonomy
A taxonomy of laboratory order codes was created. The five top-level classes of this taxonomy are miscellaneous functional tests (e.g., Coombs test and HLA screening), fluid screening tests (e.g., antibody identification and cultures), system-specific tests (e.g., tests for respiratory or gastrointestinal systems), tests for specific infections by primary manifestation (e.g., Cytomegalovirus or Lyme disease), and tests for specific noninfectious diseases (e.g., Lupus test).
This taxonomy provides a mechanism for classifying laboratory order codes systematically and for identifying agreement in mappings. Grouping laboratory orders for the same disease or pathogen enabled easy determination of the
convergence
and variations in the mapping results.
Implementation
After grouping laboratory order codes and identifying variations, additional constraints were placed on the mapping to facilitate laboratory order surveillance in a production system.
Two or more experts agreed on syndrome mapping. The consensus panel reviewed and approved the results.
Mapping was consistent in three ways as specified previously.
Specific considerations included that the fever syndrome category could be selected only if three
experts agreed because fever syndrome is more general than the other syndrome groups; the
specific infection syndrome was not selected if
a laboratory order code could be mapped to other syndromes.
Data Management
CDC BioSense receives a large amount of laboratory order data from LabCorp facilities. Many HL7 messages
are updates for the same laboratory order. Although all received messages are maintained in the data warehouse, the
most recent message of the same laboratory order is flagged for use in the BioSense web interface and for data analysis.
Results
The consensus panel's first meeting was in May 2004. In June, the simple mapping table was created in ACCESS, and
four experts volunteered to conduct the first round of mapping. Four mapping results were received and consolidated in July.
The final result was reported to the working group in September 2004.
Of 309 laboratory order codes, 246 were mapped into eight syndrome categories (Table 1). Some laboratory order
codes were mapped to more than one syndrome group. For example, laboratory
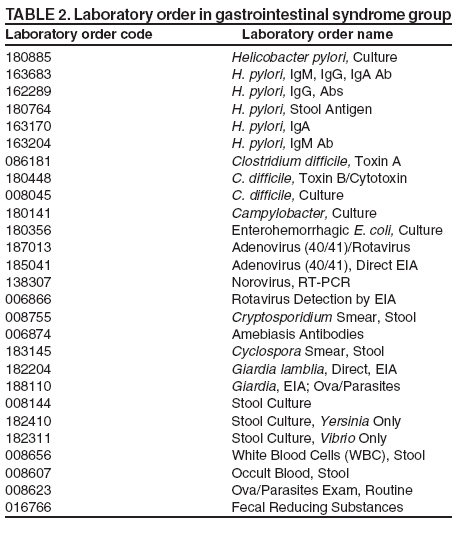
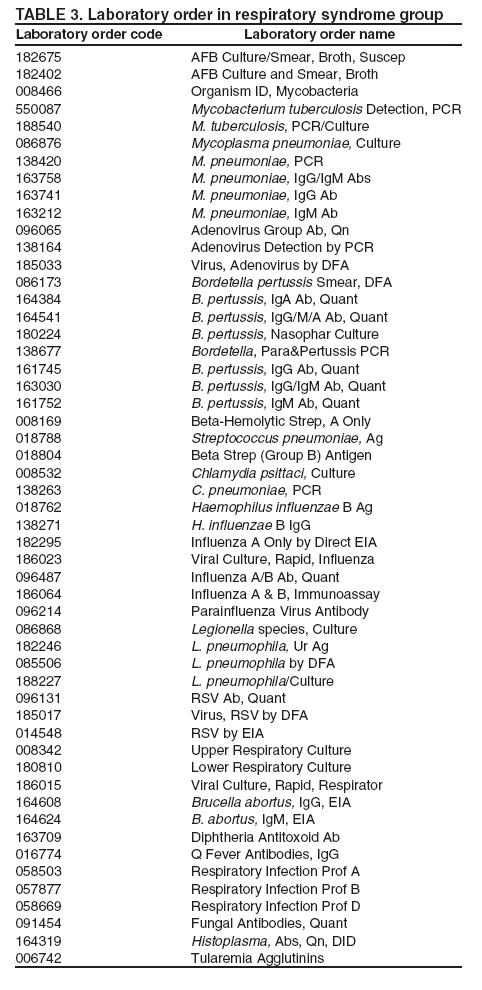
orders for tuberculosis were mapped as both fever and respiratory syndrome groups. Gastrointestinal syndrome group contains 27 laboratory order codes (Table 2). Respiratory syndrome group contains 53 LabCorp laboratory order codes (Table 3).
In addition, of 309 laboratory order codes, 63 were regarded by the working group as nonapplicable in the syndrome grouping. For example, bleeding and coagulation laboratory orders, nonspecific orders
(e.g., complete blood counts), and orders for specific purposes (HLA typing)were determined nonapplicable.
Laboratory order data have been used on the CDC BioSense surveillance production system since
November 2004. Both internal CDC BioSense monitors and state and local BioSense monitors can review the data daily for abnormal patterns. The data management team in CDC BioSense has created deduplicated data files in SAS format to facilitate data monitors' queries of records.
Discussion
Laboratory order data might provide information that can facilitate early event detection. To reduce the number
of categories under surveillance and enable the integration of laboratory orders with other surveillance data sources in BioSense, it is helpful to map laboratory order codes to syndromes before analysis.
To fully cover the received laboratory order codes, mapping was initiated with LabCorp's local codes. LabCorp has mapped most of its proprietary codes to LOINC codes. Results can be converted
to the LOINC-based mapping in the future. In the mapping process, domain experts mapped LabCorp codes directly to 11 syndromes. A laboratory order taxonomy was
applied in the consolidation phase, which helped reduce
inconsistencies. Taxonomy also provides finer granularity as
disease classifications for laboratory order codes. Disease-based classification will provide flexibility in surveillance.
This mapping process has several limitations. First, only four domain experts volunteered in the first round mapping. A larger group of experts could help the mapping results converge and
reduce inconsistency. Second, some pathogens infect
various organ systems. The precise mapping for their laboratory
order codes could only be achieved when the
specimen collected was also considered. For example,
Haemophilus influenzae could be a cause of meningitis as well as pneumonia. If
the specimen was collected from cerebrospinal fluid, this laboratory order could be mapped to the neurologicsyndrome; for a sputum sample, it would be mapped to the
respiratorysyndrome.
LabCorp messages include both laboratory order codes and ordering reasons in ICD-9-CM codes. The correlation between laboratory orders and their order reasons should be explored. Because ICD9-CM code mapping has been defined, the correlation might help improve laboratory order mapping.
With daily monitoring of laboratory order data in BioSense, the actual use of laboratory order codes in syndrome groups should be evaluated, allowing modification of mapping. Certain issues in the use of laboratory order data require
further study, such as avoiding redundancy when a series of laboratory orders, which can be grouped into the same syndrome group, was ordered on the same patient by more than one physician and defining an event when a patient received laboratory orders during a continuous period.
Conclusion
To implement the laboratory order data, laboratory order codes were mapped to syndrome groups by domain
experts a priori. In addition, a laboratory order taxonomy was created to facilitate grouping laboratory order codes and identifying inconsistencies. Finally the data management team created deduplicated data for monitors' use.
Acknowledgments
Members of the working group included John Abellera, Council of State and Territorial Epidemiologists; Martha Davis,
U.S. Department of Homeland Security; Kenneth Mandl, Harvard Medical School; Steven Babin, Joseph Lombardo, Stephen Jacob, Johns Hopkins University; David Buckeridge, Stanford Medical Informatics; Timothy Endy, Shilpa Hakre, Cara Olsen, Julie Pavlin, Walter Reed Army Institute of Research; Farzad Mostashari, New York City Department of Health and Mental Hygiene; Aaron Fleischauer, Samuel Groseclose, Mary Hamilton, Henry Rolka, Richard Hopkins, Daniel Jernigan, Haobo Ma, CDC. The authors also
appreciate LabCorp for their data provision and their consultation availability. The authors also thank Roseanne English and Paul McMurray in the CDC's BioSense BioIntelligence Center for their data management support.
References
McDonald CJ, Huff SM, Suico JG, et al. LOINC: a universal standard for identifying laboratory observations: a 5-year update. Clin Chem 2003;49:624--33.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.