 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Effect of Site of Care and Age on Timeliness and Accuracy of Syndromic Surveillance DataJohn S. Brownstein,1,2,3 K. Olson,1,2,3 K.
Kleinman,4 K. Mandl1,2,3
Corresponding author: John S. Brownstein, Division of Emergency Medicine, Children's Hospital Boston, 1 Autumn St., Rm. 542, Boston, MA 02115. Telephone: 617-355-6998; Fax: 617-730-0267; Email: john.brownstein@childrens.harvard.edu. Disclosure of relationship: The contributors of this report have disclosed that they have no financial interest, relationship, affiliation, or other association with any organization that might represent a conflict of interest. In addition, this report does not contain any discussion of unlabeled use of commercial products or products for investigational use. AbstractIntroduction: Staff of emergency and ambulatory care departments encounter data that have unique advantages for timely outbreak detection. Patient age distribution might have an effect on timeliness and accuracy of prediction. Objectives: This report identifies patient subpopulations on the basis of sites of care and patient age distribution, which signal influenza epidemics earliest and most accurately. Methods: Analyses performed included cross-sectional, time series analyses of seven patient populations comprising a health maintenance organization providing ambulatory care, three emergency departments (EDs) at urban tertiary care, and three community-based hospitals in eastern Massachusetts. Except for two EDs (one adult and one pediatric), these hospitals serve all patient age groups. Patients having respiratory infection syndromes and who visited each health-care setting during January 1, 2000-September 30, 2004, were identified and categorized by age (Figure). Cross-spectral analyses and Poisson regression models were used to evaluate timelines and prediction for New England's influenza and pneumonia mortality, as reported to CDC. Results: Patient age significantly influences timeliness of signal for influenza and pneumonia mortality (p = 0.026), with the pediatric ED patients presenting with influenza earliest in the season. In the cohorts, children aged 3--4 years consistently presented to sites of care first (p<0.05). By using regression models to predict mortality based on the time-shifted surveillance data, all cohorts were identified as significant predictors of influenza mortality. However, patient age also significantly influences level of prediction (p = 0.036). The age group of children aged <3 years can be used to predict significantly more of the variation than other age groups (p<0.05). Conclusion: Patient age is a key determinant in the timing of visits for respiratory infections. Pediatric patients seek ambulatory and emergency care before adult patients. The earliest arriving group is preschool-aged children (aged 3--4 years), who are considered predominant vectors in household spread of influenza. The age group of children <3 years can be used to best predict influenza mortality, again highlighting the importance of treating pediatric patients as sentinels. Monitoring pediatric patient subpopulations separately from other subpopulations might enhance syndromic surveillance systems. Figure 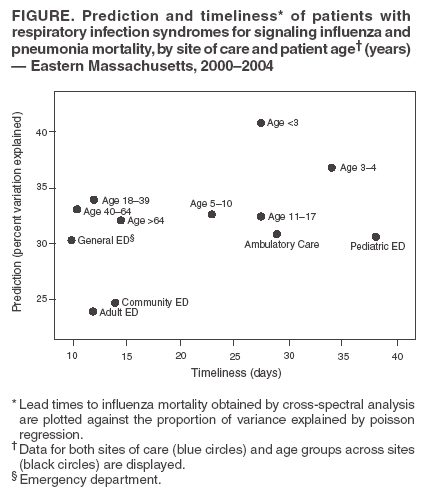 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 8/5/2005 |
|||||||||
|