 ShareCompartir
ShareCompartir
FIGURE. Timeline of events relevant to diagnosis of Ebola virus disease (Ebola) in patient 3 — Ohio and Texas, September 20–November 3, 2014
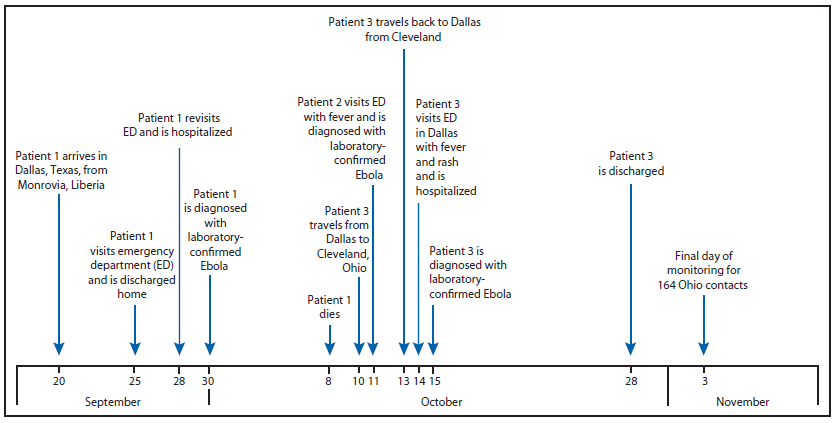
Alternate Text: The figure above is a timeline showing events relevant to diagnosis of Ebola virus disease in patient 3 in Texas and Ohio during September 20-November 3, 2014. The patient visited Ohio during October 10-13, traveling by commercial airline between Dallas, Texas, and Cleveland, Ohio.
