|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
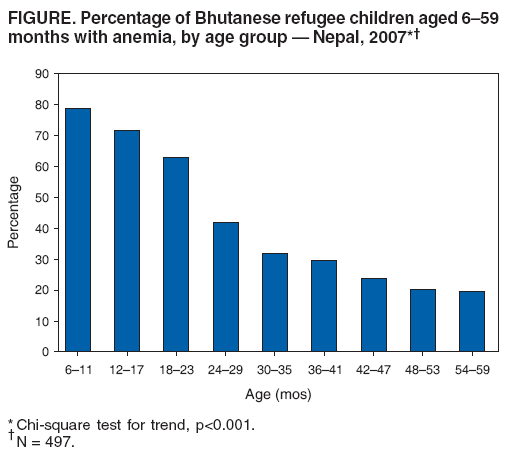
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Malnutrition and Micronutrient Deficiencies Among Bhutanese Refugee Children --- Nepal, 2007Acute and chronic malnutrition and micronutrient deficiencies have been found in refugee camp populations (1). In southeastern Nepal, despite consistent access by refugees to general rations,* certain micronutrient deficiencies have posed a substantial health burden to the approximately 100,000 Bhutanese residing in seven refugee camps (2). Limited food diversity, frequent illness, and poor feeding practices have been cited as underlying causes of poor nutritional status in this population. Annual surveys to assess levels of acute malnutrition (i.e., wasting) and chronic malnutrition (i.e., stunting) have been conducted in these camps by the Association of Medical Doctors of Asia (AMDA) and United Nations High Commissioner for Refugees (UNHCR); however, the capacity to reliably evaluate micronutrient deficiencies has not existed locally in the camps (3). In January 2007, AMDA and CDC, at the request of UNHCR and the World Food Programme (WFP), conducted a nutritional survey of children aged 6--59 months, assessing 1) the prevalence of acute malnutrition, chronic malnutrition, underweight, anemia, and angular stomatitis (i.e., riboflavin deficiency); 2) the cumulative incidence of diarrhea and acute respiratory illness (ARI); and 3) the feeding practices of the children's mothers. This report describes the results of that survey, which indicated that, although acute malnutrition was found in only 4.2% of the children, chronic malnutrition was found in 26.9% and anemia in 43.3%. These findings underscore the importance of monitoring both malnutrition and micronutrient deficiencies and addressing the underlying causes of nutritional deficits. In 1991, approximately 100,000 Bhutanese mostly of Nepali origin began fleeing ethnic persecution in Bhutan and now live in seven refugee camps in southeastern Nepal. This refugee population has been stable since 1993 but remains dependent on food assistance. During January 28--February 6, 2007, a cross-sectional survey was conducted in the Bhutanese refugee camps. The number of households selected in each camp was proportional to the size of the camp; individual households were selected using a systematic random sampling method. Information was collected regarding all children aged 6--59 months in each household by interviewing their mothers. Questions were asked regarding foods eaten by their children within the preceding 24 hours, incidence of diarrhea (i.e., three or more episodes within the preceding 24 hours) or ARI (i.e., fever plus either cough or difficulty breathing) in children within the preceding 14 days, and beliefs regarding their practices for feeding their children. In addition, the children's weight and height measurements, hemoglobin levels, and presence of clinical signs of angular stomatitis were assessed. Weight was measured using digital scales, and height (or recumbent length for children aged <2 years) was measured using a Shorr Infant-Child Height Board (4). Acute malnutrition was defined as a weight-for-height z-score <-2 or the presence of edema; severe acute malnutrition was defined as a weight-for-height z-score <-3 or edema (5). Chronic malnutrition was defined as a height-for-age z-score <-2; severe chronic malnutrition was defined as a height-for-age z-score <-3. Underweight was defined as a weight-for-age z-score <-2; severe underweight was defined as a weight-for-age z-score <-3. Hemoglobin was measured using a Hemocue B-Hemoglobin Photometer (6). Anemia was defined as hemoglobin <11.0 g/dL for children and pregnant women and <12.0 g/dL for nonpregnant women. The survey sample included 497 children and their 413 mothers. Twenty-one (4.2%) of the children aged 6--59 months had acute malnutrition, and one (0.2%) had severe acute malnutrition (Table). The prevalence of acute malnutrition was greatest (6.0%) among children aged 12--23 months. Chronic malnutrition was identified in 134 (26.9%) children, and severe chronic malnutrition was identified in 21 (4.2%) children. A total of 125 (25.1%) children were underweight, and 24 (4.8%) were severely underweight. Both chronic malnutrition and underweight increased with age (chi square for both trends: p = 0.001). Among the children, 215 (43.3%) had anemia; prevalence of anemia decreased with age (Figure), from 78.8% among infants aged 6--11 months to 20.1% among children aged 48--59 months (chi square for trend: p<0.001). Angular stomatitis was identified in 56 (11.3%) children. The reported cumulative incidence of diarrhea and ARI in children during the preceding 14 days was 30.0% and 28.8%, respectively (Table). Among the mothers, 56 (13.6%) had anemia; prevalence of anemia was significantly higher (p = 0.01) among mothers who were vegetarians (26.3%) than among nonvegetarians (12.1%). Twenty (4.9%) mothers reported exclusive breastfeeding of their children aged <6 months, and 314 (76.1%) reported introducing liquids other than breast milk to their children aged <3 months. Cumulative incidence of diarrhea and ARI, frequency of foods consumed within the preceding 24 hours, and presence of anemia in mothers were not associated with anemia among the children. However, given the high prevalence of anemia, iron supplementation was recommended for all children aged <2 years, in accordance with World Health Organization guidelines (7). Other recommendations included investigation of the causes of high incidence of diarrhea and ARI in the children and expanded education of mothers regarding recommended feeding practices, particularly exclusive breastfeeding of children aged <6 months and age-appropriate introduction of complementary foods. Reported by: F Abdalla, J Mutharia, MD, United Nations High Commissioner for Refugees, Geneva, Switzerland. N Rimal, MD, Assoc of Medical Doctors of Asia, Bhadrapur, Nepal. O Bilukha, MD, PhD, L Talley, MPH, T Handzel, PhD, National Center for Environmental Health; S Bamrah, MD, EIS Officer, CDC. Editorial Note:The nutritional status of refugees is determined by the prevalence of conditions related to both malnutrition and micronutrient deficiencies. However, historically, much attention has been paid to acute malnutrition and little attention to chronic malnutrition and micronutrient deficiencies. In the Bhutanese camps in Nepal, a stable population of refugees has been receiving a general ration that includes some fresh vegetables and fortified blended flour but does not meet requirements for key micronutrients such as iron, riboflavin, and vitamin C. Food often is brought to refugee camps from a distance and requires storage and distribution. Perishable foods, such as vegetables (particularly green vegetables), fruits, and meats often are too costly and logistically difficult to be purchased in large quantities, stored, transported, likely stored again, and then distributed to refugees. Restriction of refugee movement to participate in agriculture, forage for supplemental foods, or earn wages to buy commodities, further diminishes their ability to obtain micronutrient-rich foods not included in the general ration. Refugees in this setting have access to food markets; however, most do not have resources to afford foods rich in vitamins and minerals. Micronutrient deficiencies are not clinically identifiable until late stages, and serologic testing is logistically difficult and costly. Given their diagnostic difficulty and impact on growth and development, micronutrient deficiencies should be addressed in children at an early age. This survey found that the prevalence of anemia was high in children, particularly those aged 6--11 months. Anemia is a common clinical manifestation of micronutrient deficiency, particularly iron deficiency. The prevalence of anemia was much higher in the children than in their mothers, despite access to similar foods. Potential reasons for this include 1) inadequate numbers of iron-rich foods, 2) poor feeding practices, and 3) frequent episodes of common diseases, such as those causing diarrhea and respiratory infections, which can increase loss of micronutrients. Because options for diversification of the general ration are limited, diet supplementation and/or food fortification are the most likely methods to prevent micronutrient deficiencies. However, both fortification and supplementation are costly, and the addition of some fortificants reduces the shelf-life of commodities (8). Implementing supplementation and fortification programs will require changes in policies and practices of food aid agencies and increased donor participation, although fortification often is a cost-effective strategy for addressing micronutrient problems. Educating mothers regarding appropriate breastfeeding and complementary feeding practices also is critical to preventing anemia and malnutrition in young children. Appropriate feeding practices include both exclusive breastfeeding until age 6 months and introduction of complementary foods rich in vitamins and minerals at appropriate ages. Exclusive breastfeeding until age 6 months is nutritionally adequate, protects children against infection, and prevents introduction of liquids, such as tea, that can inhibit iron absorption (9). The high incidence of illness, particularly diarrheal disease, in these children can decrease absorption and increase loss of micronutrients while also increasing metabolic (and consequently micronutrient) requirements. Determining the causes of frequent illnesses in the Bhutanese refugee children and implementing appropriate interventions to address these causes can decrease the effects of morbidity on micronutrient deficiencies and overall nutritional status (10). The findings in this report are subject to at least one limitation. Although anemia was evaluated as a marker for iron deficiency, levels of iron deficiency (e.g., ferritin or transferrin receptors) were not measured directly. In addition, other clinically relevant micronutrients, such as thiamine, vitamin A, or zinc, were not measured because of cost and logistical constraints. Additional priority given to chronic malnutrition and micronutrient deficiencies in refugee camps might reduce the incidence of anemia and other potential sequelae of these conditions, including slowed growth and development. One strategy that has been shown to reduce anemia in children and is currently being evaluated in refugee camp settings is the use of Sprinkles®,† packets of dry powder, containing iron and other micronutrients intended for home fortification of foods. As lengths of stay in refugee camps increase, agencies should consider this and other new strategies to address all possible negative nutritional outcomes of prolonged dependence on food aid. Acknowledgment This report is based, in part, on contributions by S Mukherjee, World Food Programme, Damak, Nepal. References
* A daily general ration in Bhutanese refugee camps in Nepal consists of parboiled rice, 400 g; whole grain, 20 g; lentils, 40 g; vegetable oil, 25 g; sugar, 20 g; wheat soya blend, 35 g; salt, 7.5 g; fresh vegetables, 260 g (rotated each month and including cauliflower, potato, pumpkin, squash, and radish). † Additional information available at http://www.sghi.org/about_sprinkles/index.html. Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/9/2008 |
|||||||||
|