|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
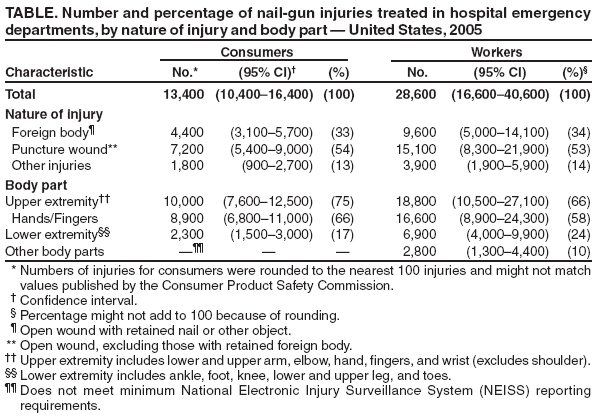
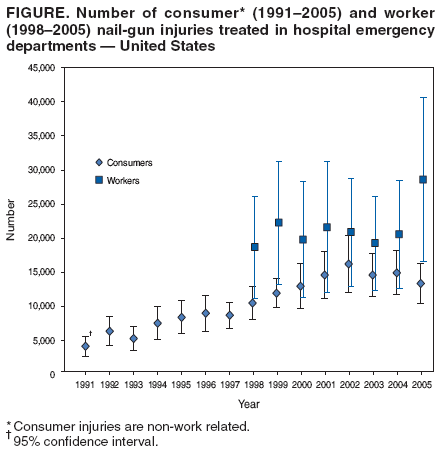
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nail-Gun Injuries Treated in Emergency Departments --- United States, 2001--2005Speed, ease of use, and ready availability have made pneumatic nail guns a common tool used in work settings such as residential construction and wood-product fabrication. In addition, the tools are now readily available to consumers, extending to the public what had been primarily a potential work-related hazard. To characterize nail-gun injuries in work and nonwork settings, patients with nail-gun injuries treated in U.S. hospital emergency departments (EDs) were studied by using the U.S. Consumer Product Safety Commission's (CPSC's) National Electronic Injury Surveillance System (NEISS) and the NEISS occupational injury supplement (NEISS-Work) maintained by CDC's National Institute for Occupational Safety and Health (NIOSH). This report describes the results of that analysis, which indicated that during the 5-year period 2001--2005, an average of approximately 37,000 patients with injuries* related to nail-gun use were treated annually in EDs, with 40% of injuries (14,800) occurring among consumers.† In addition, data on ED-treated injuries indicated that, in 2005, nail-gun injuries among consumers were approximately three times higher than in 1991 (4,200). Additional measures are needed to prevent nail-gun injuries among both workers and consumers. Nail-gun injury estimates for consumers were obtained from CPSC's online NEISS data (1); NEISS data are derived from a national stratified probability sample of 101 U.S. hospital EDs (2). Estimates for work-related nail-gun injuries were taken from NEISS-Work, an adjunct occupational injury and illness surveillance program with a 67-hospital sample (3).§ An injury was identified as work related if the ED chart indicated that the injury occurred while working for pay or other compensation, while volunteering for an organized group, or during agricultural production-related activities. Consumer nail-gun injuries were defined as ED-treated injuries that involved "nail guns or stud drivers" (CPSC product code 0882), excluding heavy-duty staplers (CPSC product code 0834) (1). The CPSC online NEISS data system produced the national estimates with variances (used to calculate 95% confidence intervals [CIs]) (1); individual consumer case records were not reviewed. Cases were weighted on the basis of the size (i.e., annual number of ED visits) of the hospital in which treatment was received. The number of injuries was the sum of the case weights, and variances were calculated using the classic formula for the variance of a total from a stratified sample. Work-related nail-gun injuries were identified from NIOSH NEISS-Work data as those involving pneumatic nail guns and excluding heavy-duty staplers, rivet drivers, and electric or powder-actuated tools. Nail-gun injuries were identified based on CPSC product code 0882, the Occupational Injury and Illness Classification System injury and illness source/secondary source code 7291 (nail guns --- powered) (4), and key words (e.g., nail gun, nailer, shot, or gun) from case narratives. Injuries included being shot by a nail from a gun, being struck by the nail gun or the hose from a compressor, and reporting either a musculoskeletal injury or an eye injury associated with use of the nail gun. Work-related injury estimates and variances were calculated by the same methods used by CPSC for consumer-product--related injuries (1). Consumer-product--related injuries and work-related nail-gun injuries were mutually exclusive. During 2001--2005, annual consumer nail-gun injuries ranged from 13,400 to 16,200, with an annual average of 14,800 ED-treated injuries (Figure). During the same period, work-related nail-gun injuries ranged from 19,300 to 28,600, with an annual average of 22,200. A steady increase in injuries among consumers occurred during the 1990s. Similar data for workers were not available before 1998. In 2005, approximately 12,800 (96%) of 13,400 consumers injured by nails guns and 28,000 (98%) of 28,600 workers injured by nail guns were men. Injured workers had a median age of 27 years, and consumers had a median age of 35 years. For both consumers and workers, the diagnosis associated with 87% of the nail-gun injuries was either wound with a foreign body (i.e., open wound with retained nail or other object) or puncture wound (i.e., open wound, excluding those with retained foreign body) (Table). Certain puncture wounds resulted from a nail going through construction material into a person; in others, a nail was shot completely through a body part, or a person removed the nail before seeking treatment. Approximately 4% of nail-gun injuries among workers resulted in fractured bones.¶ Injuries to upper extremities, primarily hands and fingers, accounted for 75% of all consumer nail-gun injuries and 66% of all worker nail-gun injuries. Lower extremities also were injured frequently, accounting for 17% of consumer injuries and 24% of worker injuries. Examples of other nail-gun injuries among either workers or consumers included eye injuries from foreign bodies and corneal abrasions; dental injuries; musculoskeletal injuries such as sprains, strains, tendonitis, nerve damage from tool use, and finger dislocation from reaching and lifting a tool; lacerations; electrical burns; and noise-induced hearing difficulty.** Among 1,500 workers hospitalized for nail-gun injuries in 2005 (CI = 700--2,200), approximately 60% had foreign-body injuries and 35% had puncture wounds,†† whereas overall, more persons had puncture wounds than foreign-body injuries (Table). Wounds requiring hospitalization included embedded nails in the trunk, head, joints, or bones; fractures from nail penetration; and infected puncture wounds. Most persons with nail-gun injuries were not hospitalized; 12,600 (94%) consumers and 26,900 (94%) workers were treated and released from EDs in 2005. Reported by: HJ Lipscomb, PhD, Div Occupational and Environmental Medicine, Dept Community and Family Medicine, Duke Univ Medical Ctr, Durham, North Carolina. LL Jackson, PhD, Div of Safety Research, National Institute for Occupational Safety and Health, CDC. Editorial Note:Since 1991, annual consumer nail-gun injuries have increased approximately 200%. This increase likely corresponds to an increase in availability during the 1990s of inexpensive pneumatic nail guns and air compressors (used to power the nail guns) in home hardware stores; however, no sales data are available for confirmation. The number of worker nail-gun injuries has remained stable since 1998 (when data comparable to those for consumers became available), with the exception of 2005. In 2005, the estimated number of nail-gun injuries among workers increased 39% from 2004. This increase was distributed uniformly throughout the year, and the reason for the increase is unclear. Although the increase is not statistically significant (p>0.05) compared with estimates for the preceding years, the change indicates a need for close monitoring. Nail guns in the consumer and commercial markets differ, but similar models are available in both markets. The current national standard for pneumatic fastener driving tools (American National Standards Institute [ANSI] SNT-101-2002) applies to products in both markets (5). According to the ANSI standard, actuation (firing) mechanisms on nail guns have two critical components to prevent unintentional firing: a manual trigger and a contact element in the nose of the gun. The most common type of firing mechanism is the dual-action contact-trip trigger, which requires that the manual trigger and nose contact element both be depressed for a nail to be discharged. When users depress the manual trigger, they can rapidly fire a nail (i.e., "bounce nail") each time the nail-gun nose contacts the work material, speeding up production. Trigger locks and other user modifications that keep the trigger constantly depressed or that disable the nose contact switch have been used to make rapid nailing easier, but this counteracts the safety features of the dual-action contact-trip mechanism. Another type of firing mechanism, the alternative sequential-trip trigger, requires the nose contact to be depressed before the manual trigger, rather than simultaneously with the trigger, to discharge a nail, making unintentional discharge of nails less likely. Injury surveillance in the residential construction industry has indicated that approximately 65%--69% of injuries from contact-trip tools likely could be prevented through use of a sequential-trip trigger (6--8). The International Staple, Nail, and Tool Association adopted a voluntary ANSI standard recommending that manufacturers install sequential-trip triggers on certain types of nail guns before distribution, beginning in May 2003 (5); however, under the standard, contact-trip triggers can continue to be sold with nail guns or as an option. The findings in this report are subject to at least four limitations. First, the total number of injuries from nail guns is underrepresented by NEISS because the system only counts injuries treated in EDs; however, EDs are likely to treat a high proportion of nail-gun puncture wounds and embedded nails. In addition, only the most severe injury at the time of treatment is recorded for an individual person; a single incident might have resulted in multiple injuries or more severe sequelae. Second, the identification of cases and their specific characteristics is limited by the availability of appropriate information in the ED records and subsequent reporting by the hospital records abstractors. Thus, misclassification might have occurred in describing the person who was injured (consumer versus worker), the type of fastener tool, and the injury diagnosis (foreign-body versus puncture wound). Third, the small hospital sample size resulted in large standard errors (10%--20%) that might have obscured significant differences among years. CIs for work-related injury estimates are larger than for consumer injuries because of the smaller hospital sample used for data collection. Finally, NEISS ED surveillance does not provide information about the population at risk, the amount of exposure (e.g., hours of tool use), or tool characteristics (e.g., type of nail gun or trigger mechanism). Although consumers had fewer injuries than workers during 2001--2005, if consumers had substantially fewer hours of exposure (i.e., tool use) than workers, consumer nail-gun injury rates might have been higher than those of workers. NEISS consumer injury estimates and NEISS-Work occupational injury estimates provide a national perspective on the injuries received from nail guns and indicate how injuries from tools used in work and nonwork settings can overlap (9). Although training regarding safe work practices might reduce nail-gun injuries, use of sequential-trip triggers is likely to be more effective (6--8), particularly among consumers, who do not usually receive training in tool use. The voluntary ANSI standard only addresses availability of the sequential-trip triggers and does not address the continued use of contact-trip triggers. The ANSI standard revision is likely to decrease injuries over time as older tools with contact-trip triggers are no longer being sold or used, but perceived lack of future availability might result in the contact-trip trigger tools being retained in work settings. In addition, consumers might be unaware of the need to replace older contact-trip triggers with sequential-trip triggers. Therefore, distribution of new nail guns with sequential-trip triggers and availability in home hardware centers of kits to convert contact-trip triggers to sequential-trip triggers might help reduce the use of the more hazardous tools. Moreover, additional training material on nail-gun safety to supplement product information included with the tools should be provided at the point of sale or rental to further influence safe nail-gun use among consumers and workers. Acknowledgments This report is based, in part, on data contributed by T Schroeder, CPSC Division of Hazards and Injury Data Systems; and NEISS hospital ED record abstractors. References
* For this report, all cases are referred to as injuries; however, ED-treated illnesses and disorders are included in the national estimates. Among the NEISS-Work cases, 90%--95% of the cases are injuries. Although NEISS programs collect information on injuries and illnesses (e.g., infection of a nail-gun wound or repetitive motion disorder), they are not categorized separately in the available data. † All references to consumers and consumer-product injuries are nonwork related. § The NEISS-Work sample for occupational injuries uses 67 of the 101 NEISS hospitals used by CPSC for consumer-product--related injuries. The 67-hospital sample is distributed proportionately across the strata similar to the larger CPSC sample and statistically weighted to appropriately account for the smaller sample size. Because of hospital closures and other nonparticipation and nonresponse factors, the number of reporting hospitals can vary monthly and yearly. ¶ Number of fractures did not meet minimum NEISS reporting requirements because the national estimate was too small, the coefficient of variation exceeded 33%, or both. Percentages are provided for information purposes only and might be unstable. ** National estimates did not meet minimum NEISS reporting requirements because the national estimate was too small, the coefficient of variation exceeded 33%, or both. †† Number of persons hospitalized as a result of foreign-body or puncture wounds did not meet minimum NEISS reporting requirements because the national estimate was too small, the coefficient of variation exceeded 33%, or both. Percentages are provided for information purposes only and might be unstable. Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/12/2007 |
|||||||||
|