|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
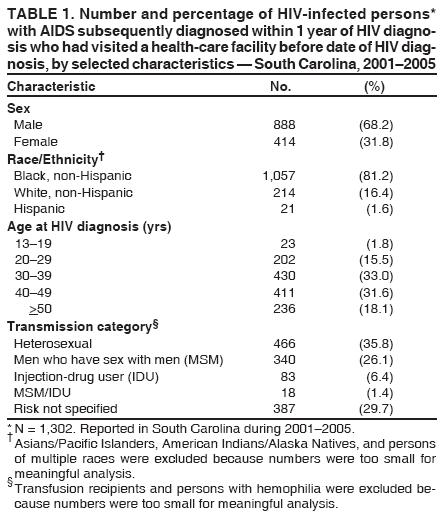
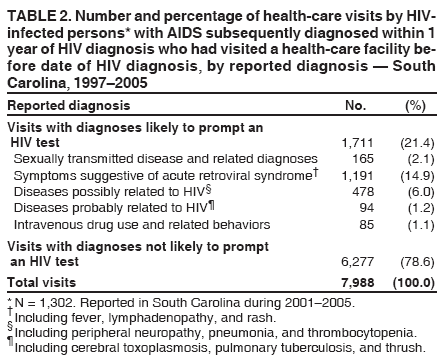
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Missed Opportunities for Earlier Diagnosis of HIV Infection --- South Carolina, 1997--2005In September 2006, CDC published revised recommendations for human immunodeficiency virus (HIV) testing in health-care settings to 1) increase early detection of HIV infection by expanding HIV screening of patients and 2) improve access to HIV care and prevention services (e.g., by conducting screening in locations such as emergency departments and urgent-care facilities, where persons who do not otherwise access HIV testing seek health-care services) (1). HIV screening is now recommended for patients aged 13--64 years in all health-care settings after patients are notified that testing will be performed unless they decline (opt-out screening). This represents a substantial change from earlier recommendations to 1) offer HIV testing routinely to all patients only in health-care settings with high HIV prevalence and 2) conduct targeted screening on the basis of risk behaviors for patients in low-prevalence settings (2). This report examines HIV and acquired immunodeficiency syndrome (AIDS) case reporting in South Carolina before the 2006 recommendations were published. During 2001--2005, a total of 4,315 cases of HIV infection were reported in South Carolina. Of these, 41% were in persons (referred to as late testers) in whom AIDS was diagnosed within 1 year of their initial HIV diagnosis* (4). Of these late testers, 73% made a total of 7,988 visits to a South Carolina health-care facility during 1997--2005 before their first reported positive HIV test. The diagnoses reported for 79% of these visits were not likely to prompt HIV testing under a risk-based testing strategy. These findings suggest that routine, opt-out HIV screening of all patients in health-care settings, rather than risk-based HIV testing, might result in substantially earlier HIV diagnoses in South Carolina. HIV/AIDS cases have been reportable by patient name in South Carolina since 1986. This analysis used data from the South Carolina HIV/AIDS Reporting System (HARS) for 2001--2005 and included date of first HIV-positive test, date of AIDS diagnosis, and state of residence. Data quality from HARS exceeds CDC minimum standards on reporting timeliness (95% of cases reported within 6 months of a diagnosis) and completeness of reporting (98%, based on a comparison with other data sources) (South Carolina Department of Health and Environment Control [DHEC], unpublished data, 2005). Since 1996, state law has required that the Office of Research and Statistics (ORS), South Carolina Budget and Control Board receive reports on all diagnoses (classified by International Classification of Diseases [ICD] codes) from all emergency departments, hospital inpatient facilities, ambulatory-care facilities, and outpatient surgery facilities within the state. The health-care data for this report were supplied by 60 emergency departments, 62 inpatient facilities, 63 ambulatory-care facilities or outpatient surgery facilities, and 19 free medical clinics in the state, and represent visits that occurred during 1997--2005. ICD diagnoses were grouped into two categories: 1) diagnoses not suggestive of HIV infection and unlikely to have prompted an HIV test (e.g., hypertension, diabetes, and constipation) and 2) diagnoses suggestive of HIV infection that should have prompted an HIV test (e.g., sexually transmitted diseases, symptoms suggestive of acute retroviral syndrome [5], intravenous drug use, and diseases possibly or probably related to HIV infection [6]). Data from HARS and ORS were linked using several identifiers, including patient name, date of birth, sex, race/ethnicity, and county of residence. This use of the data was approved by DHEC and the ORS Data Oversight Committee. The data were matched in a secured location by authorized persons who were trained in HARS security and confidentiality guidelines. All identifiers were removed from the analysis dataset provided to investigators, who also signed confidentiality agreements. During 2001--2005, a total of 4,315 persons with HIV infection in South Carolina were reported to HARS, of whom 1,784 (41.3%) were late testers, including 710 (16.5%) who had AIDS diagnosed within 30 days of their initial HIV diagnoses. Women were less likely than men to be late testers; other demographic and risk characteristics of late testers were similar to those of persons reported to HARS who did not have onset of AIDS within 1 year of their HIV diagnoses. Of the 1,784 late testers, 1,302 (73.0%) had at least one documented visit to a South Carolina health-care facility during 1997--2005 and before the reported date of HIV diagnosis (Table 1). A total of 7,988 health-care visits were recorded for the 1,302 late testers who had previously visited a health-care facility. Information on transmission category indicated that 441 (33.9%) of these 1,302 persons were identified as injection-drug users or men who have sex with men, persons with high-risk practices that should have prompted HIV screening if risk histories had been elicited during the health-care visits. However, diagnoses reported for 6,277 (78.6%) of these visits were not likely to prompt an HIV test (Table 2). Of the 7,988 visits, 6,303 (78.9%) were to emergency departments, 982 (12.3%) to inpatient settings, 594 (7.4%) to outpatient facilities, and 109 (1.4%) to free clinics. The median time between the visit to a health-care facility and the date of HIV diagnosis was 2.5 years (range: 0--9 years). The 1,302 late testers made a median of four health-care visits before HIV diagnosis (range: 1--132 visits); 280 (21.5%) late testers made only one health-care visit before HIV diagnosis, 567 (43.5%) made two to five previous visits, 259 (19.9%) made six to 10 visits, and 196 (15.1%) made more than 10 visits. Visits occurring <6 months before HIV diagnosis accounted for 1,202 (15.1%) of the 7,988 visits; 818 (10.2%) of visits were made >6 months to 1 year before, 1,340 (16.8%) were >1 to 2 years before, 1,337 (16.7%) were >2 to 3 years before, and 3,291 (41.2%) were >3 years before HIV diagnosis. Reported by: W Duffus, MD, L Kettinger, MPH, T Stephens, MSPH, J Gibson, MD, South Carolina Dept of Health and Environmental Control; K Weis, MPH, School of Public Health, Univ of South Carolina; M Tyrell, PhD, D Patterson, PhD, C Finney, MPH, WP Bailey, MPH, Office of Research and Statistics, South Carolina Budget and Control Board. B Branson, MD, L Gardner, PhD, PH Kilmarx, MD, Div of HIV/AIDS Prevention, National Center for HIV, Viral Hepatitis, STDs, and Tuberculosis Prevention (proposed), CDC. Editorial Note:The findings in this report indicate that HIV-testing practices in South Carolina failed to identify a substantial proportion of HIV-infected persons early in the course of their infection. Early diagnosis of HIV infection is beneficial to the health of the patient (7) and might have a role in limiting further HIV transmission (8). Among the persons identified in this report as late testers (i.e., persons who received an AIDS diagnosis within 1 year of HIV diagnosis), approximately three fourths had visited a South Carolina health-care facility before having HIV diagnosed. Most of the late testers made multiple visits, and most of their visits occurred 1 year or more before diagnosis of HIV infection. These health-care encounters represent missed opportunities for earlier HIV diagnosis. The majority of diagnoses for these previous visits probably would not have prompted HIV testing under a risk-based testing strategy. In addition, the information on transmission category indicated that 441 (33.9%) of 1,302 persons were identified as injection-drug users or men who have sex with men, persons with high-risk practices that should have prompted HIV screening. Combined, these findings support the new recommendations for routine, opt-out HIV screening of patients in all health-care settings. In 2004, South Carolina ranked tenth in rate of annual reported AIDS cases in the United States, with 18.1 AIDS cases per 100,000 population (9). The state's data on persons with newly diagnosed HIV in 2004--2005 indicate that a substantial proportion had low CD4+ T cell counts, which would have qualified them for antiretroviral treatment; nearly one third had <200 cells per mm3, and approximately half had <350 cells per mm3 (DHEC, unpublished data, 2006). These data also suggest a high prevalence and long duration of undiagnosed HIV infections in South Carolina. The findings in this report are subject to at least five limitations. First, although HARS and ORS data are comprehensive, certain HIV/AIDS diagnoses and health-care visits probably were not reported. Second, although several variables were available for linking records between the two datasets, matching might not have been successful in all cases. Third, certain late testers might not have been HIV infected at the time of the previous health-care encounters, some of which occurred up to 8 years before AIDS was diagnosed; therefore, those instances might not have been missed opportunities for HIV diagnosis. However, given the long average latent period of approximately 10 years after HIV infection before the onset of AIDS (3), most persons who had AIDS during 2001--2005 would already have been HIV infected during most of their health-care visits beginning in 1997. Fourth, HIV testing might have been recommended but rejected by certain patients during earlier visits; refusal to test might have been related to the stigma that can be associated with risk-based HIV testing. Finally, referral for HIV testing might have occurred during some of the health-care encounters before HIV was diagnosed, so these visits might not represent missed opportunities. Given the substantial number of health-care encounters in South Carolina during which an earlier diagnosis of HIV might have been made and the high proportion of these visits that would not have suggested the benefit of an HIV test under the risk-based HIV-testing strategy, these findings underscore the need for routine HIV screening of adults and adolescents visiting health-care facilities. The capacity of treatment and preventive services will need to be increased if HIV testing is made routine. Efforts are ongoing in South Carolina to expand these services. The benefit of routine HIV screening, early diagnosis of HIV infection, and linkage of infected persons to these services might be considerable because previous practices of testing based on risk factors or symptoms did not identify a substantial proportion of HIV-infected persons until late in the course of their disease. References
* The average latent period from HIV infection to onset of AIDS is approximately 10 years (3).
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/29/2006 |
|||||||||
|