|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
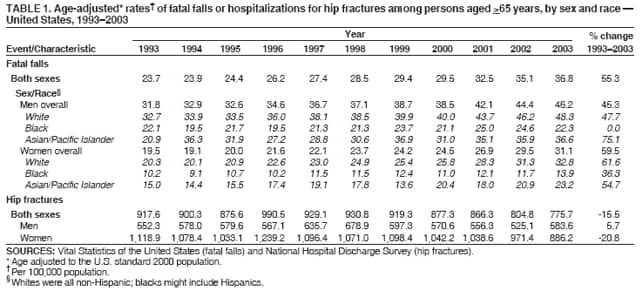
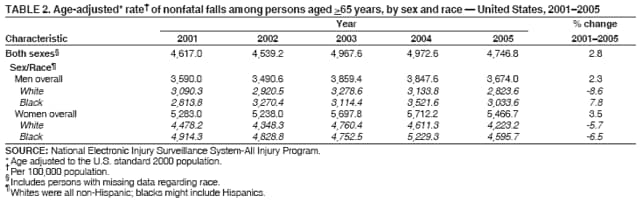
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Fatalities and Injuries from Falls Among Older Adults --- United States, 1993--2003 and 2001--2005Unintentional falls are a common occurrence among older adults, affecting approximately 30% of persons aged >65 years each year (1). The injuries received from a fall can result in death, disability, nursing-home admission, and direct medical costs (2,3). In 2003, a total of 13,700 persons aged >65 years died from falls, and 1.8 million were treated in emergency departments (EDs) for nonfatal injuries from falls.* Falls cause the majority of hip fractures, which often result in long-term functional impairments that might require admission to a nursing home for a year or more (2). To examine trends in fatal and nonfatal falls among older persons, CDC analyzed U.S. rates of 1) fatalities from falls (during 1993--2003), 2) hospitalizations for hip fractures (1993--2003), and 3) nonfatal injuries resulting from falls in persons treated in EDs (2001--2005). This report summarizes the results of those analyses, which indicated that, during 1993--2003, the overall rate of fatal falls among persons aged >65 years increased, and the rate of hospitalizations for hip fractures decreased; during 2001--2005, the change in the overall rate of nonfatal injuries from falls was not statistically significant. However, disparities by sex existed for all three measures. Certain interventions can reduce falls (e.g., exercising regularly or having medicines reviewed to reduce side effects and interactions), but implementation at the community level remains limited (2), and additional measures are needed to promote widespread adoption. Data on fatal falls that occurred during 1993--2003 were obtained from annual mortality data of the Vital Statistics of the United States (4). Cause-of-death data were based on information from death certificates completed by attending physicians, medical examiners, or coroners. Fall-related deaths for 1993--1998 were defined as those deaths with an underlying cause coded E880--E886.9 or E888, according to the International Classification of Diseases, Ninth Revision (ICD-9); for 1999--2003, fall-related deaths were defined as those deaths coded W00--W19 according to the Tenth Revision (ICD-10) (5). National estimates of hospital admissions for hip fractures that occurred during 1993--2003 were obtained from the National Hospital Discharge Survey (NHDS), which collects data from a sample of inpatient records acquired from a national probability sample of nonfederal, short-stay hospitals; data represent a sample of hospital discharges. Hospitalizations for hip fractures include cases with any diagnosis coded 820, according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) (6). Data on nonfatal injuries from falls that occurred during 2001--2005 were obtained from the National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP), which is operated by the Consumer Product Safety Commission and collects data regarding initial visits for all types and causes of injuries in persons treated in EDs. These data are drawn from a nationally representative sample of 66 hospitals, selected as a stratified probability sample of hospitals in the United States (7). Information about the most severe injury for each case is collected from the medical record; data are weighted by the inverse probability of selection and summed to produce national estimates. Denominators for rates of fatal falls, hip fractures, and nonfatal injuries from falls were calculated using U.S. Census population estimates,† and rates were age adjusted to the 2000 U.S. standard population. Weighted least squares regression was used to test for linear trend (as the percentage change in annual rates); differences with p<0.05 were considered statistically significant (8). During 1993--2003, the age-adjusted rate of fatalities from falls increased significantly, and rates were significantly higher among men compared with women (Table 1). Fatality rates increased both for men (from 31.8 per 100,000 population to 46.2, an increase of 45.3%) (p<0.01) and women (from 19.5 per 100,000 population to 31.1, an increase of 59.5%) (p<0.01). During 1993--2003, rates increased in all racial populations for both sexes, with the exception of black men, whose rate was unchanged. In 2003, rates varied by race among both men (whites: 48.3 per 100,000 population; Asians/Pacific Islanders [A/PI]: 36.6; and blacks: 22.3) and women (whites: 32.8 per 100,000 population; A/PI: 23.2; and blacks: 13.9). During 1993--2003, the overall age-adjusted hospitalization rate for hip fractures decreased by 15.5%, from 917.6 per 100,000 population to 775.7 (p = 0.001 test for trend) (Table 1). The hospitalization rate increased to 990.5 per 100,000 population during 1993--1996, before declining. During 1993--2003, rates differed by sex. The annual rate for women was 52%--119% higher than the rate for men. However, the hospitalization rate for hip fractures did not increase significantly (5.7%, p = 0.53) for men during 1993--2003 and declined 20.8% (p<0.01) for women. During 2001--2005, neither the change in the overall rate of nonfatal injury from falls nor any of the changes by sex or race were significant (Table 2). In contrast to fatal falls, annual rates of nonfatal injuries for women were, on average, 48.4% higher than the rates for men. Comparing rates for fatal falls and nonfatal injuries from falls during the most recent 3-year period (2001--2003) when data for both were available, the rate for fatal falls increased 13.3% (9.8% for men and 15.6% for women), whereas the rates for nonfatal injuries increased 7.6% (7.5% for men and 7.9% for women). Reported by: JA Stevens, PhD, Div of Unintentional Injury Prevention; G Ryan, PhD, Office of Statistics and Programming; M Kresnow, MS, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. Editorial Note:This study examined trends in rates of fatal falls and hospitalizations for hip fractures during 1993--2003 and in rates of nonfatal injuries resulting from falls during 2001--2005. The findings indicate that rates of fatal falls increased significantly among both men and women but were consistently higher among men. Whites had the highest fatal fall rates, but an increasing trend was observed for all races. Changes in rates for nonfatal injuries from falls were not statistically significant. Although only 3 years of rates for fatal falls and nonfatal injuries could be compared directly, the greater increase in the fatal falls rate can be partly explained by the increase in injury-causing falls overall. In addition, although fatal fall rates are age adjusted, residents of the United States are living longer in large part because of decreasing mortality from chronic conditions (e.g., heart disease, cancer, or stroke). The U.S. life expectancy increased from 75.5 years in 1993 to 77.6 years in 2003 (9). These changes have resulted in a U.S. population with a greater proportion of older adults who are living with chronic diseases, leaving them at greater risk for falling and less likely to survive the injuries resulting from a fall. Rates of nonfatal injuries from falls and particularly rates of hospitalizations for hip fractures were higher among women than men. However, hospitalization rates for hip fractures appear to be declining among women. Older women are disproportionately affected by osteoporosis, a disease in which bones become porous and susceptible to fracture (2). In recent years, osteoporosis screening for women and effective treatments to rebuild bone mass have become widespread (10). These public health measures might be reflected in the lower rates for fractures. Men tend to have greater bone mass and consequently less risk for hip fractures. However, men do sustain hip fractures, especially after age 80 years; the hip-fracture rate among men has not decreased and might be increasing. Screening and osteoporosis treatment might be broadened to include older men. The findings in this report are subject to at least five limitations. First, three different data sources were used for the three rates analyzed (i.e., fatalities from falls, hospitalizations for hip fractures, and nonfatal injuries from falls in patients treated in EDs); therefore, these data might not be comparable. Second, racial categories used to analyze fatalities and nonfatal injuries differed. Third, only 5 years of NEISS-AIP data were available; therefore, the same period analyzed for fatality and hip fracture rates could not be used for nonfatal injuries from falls. Fourth, the rate of nonfatal injuries from falls likely was underestimated because only persons treated in hospital EDs were included and not those treated in outpatient settings such as clinics or physician offices. Finally, NHDS reports the number of hospital admissions, not patients; therefore, certain persons seeking treatment for hip fractures might have been counted more than once. Research has identified interventions that can reduce falls, but development and implementation of community-based programs remains limited (2). Additional measures are needed to successfully disseminate effective fall-prevention programs and to promote widespread adoption at the local level. To help prevent falls among older adults, CDC, in partnership with the CDC Foundation and MetLife Foundation, has produced four posters and updated and redesigned two brochures. What YOU Can Do to Prevent Falls outlines four key fall-prevention strategies: exercising regularly, having medications reviewed to reduce side effects and interactions, having yearly eye examinations, and reducing fall hazards in the home. Check for Safety: A Home Fall Prevention Checklist for Older Adults guides readers through a room-by-room check of their homes to find and fix hazards that can increase the risk for falling. The brochures and posters are offered in English, Spanish, and Chinese and are available at http://www.cdc.gov/ncipc/pub-res/toolkit/brochures.htm. Additional information about CDC's fall-prevention activities is available at http://www.cdc.gov/ncipc/pub-res/toolkit/toolkit.htm. References
* Web-based injury statistics query and reporting system. Available at http://www.cdc.gov/ncipc/wisqars. † U.S. Census Bureau population projections. Available at http://www.census.gov/population/www/projections/popproj.html.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/15/2006 |
|||||||||
|