 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Preventive-Care Practices Among Adults with Diabetes --- Puerto Rico, 2000--2002Preventive-care practices among persons with diabetes can prevent or delay complications such as eye disease, kidney disease, or nerve damage that is a precursor to disabling foot disease (1,2). However, the level of diabetes-related preventive care is inadequate in the United States (3--6), and little has been reported about preventive care in Puerto Rico, where an estimated 10% of adults have diagnosed diabetes (7). CDC analyzed data from 2000, 2001, and 2002 Behavioral Risk Factor Surveillance System (BRFSS) surveys to assess the percentage of adults with diabetes in Puerto Rico who engaged in five selected preventive-care practices. This report summarizes the results of that analysis, which indicated that, with the exception of hemoglobin A1c testing, the percentages of adults engaging in preventive-care practices were lower than the target percentages* set by U.S. national health objectives for 2010 (8). BRFSS conducts state-based, random-digit--dialed telephone surveys of the U.S. civilian, noninstitutionalized population aged >18 years in all 50 states, the District of Columbia, Puerto Rico, and other U.S. territories. For this analysis, respondents were considered to have diabetes if they answered "yes" to the question, "Has a doctor ever told you that you have diabetes?" Women who were told they had diabetes, but only during pregnancy, were classified as not having diabetes. Persons who reported they had diabetes were asked questions from the BRFSS diabetes module on preventive-care practices, including: "About how many times in the past 12 months has a health professional checked you for hemoglobin A1c?" "When was the last time you had an eye exam in which the pupils were dilated?" "About how many times in the last year has a health professional checked your feet for any sores or irritations?" "Have you ever taken a course in how to manage your diabetes yourself?" and "About how often do you check your blood for glucose or sugar?" The response rate to the BRFSS survey in Puerto Rico was 65.3% in 2000, 81.5% in 2001, and 75.2% in 2002. Data were aggregated for 2000--2002 to obtain reliable estimates and weighted to reflect the age and sex distribution of the Puerto Rican population. The percentages of persons with diabetes who engaged in each of the five preventive-care practices as frequently as recommended (i.e., hemoglobin A1c testing at least twice a year, eye and foot examinations at least annually, formal diabetes education ever, and self-monitoring of blood glucose [SMBG] at least daily) were age-adjusted to the 2000 U.S. standard population for comparison with U.S. national health objectives for 2010 (8). Percentages were calculated for specific age and sex groups, and a t-test was performed to determine whether differences between groups were statistically significant. In addition, the total number of preventive-care practices per person was examined. For all analyses, statistical software was used to obtain standard errors and calculate 95% confidence intervals (CIs). During 1998--2002, 10.0% of adults in Puerto Rico had diagnosed diabetes; prevalence was highest (25.3%) among those aged >65 years (7). However, during 2000--2002, the percentages of adults with diabetes in Puerto Rico who engaged in preventive-care practices as frequently as recommended, with the exception of hemoglobin A1c testing, were lower than U.S. national health objectives for 2010 (Figure 1). The age-adjusted percentage for hemoglobin A1c testing at least twice a year was 67.3%, compared with the national target of 65%. Age-adjusted percentages for annual eye and foot examinations were 54.6% and 45.6%, respectively, versus the target of 75% for both practices; percentages for ever having received diabetes self-management education and for daily SMBG were 28.1% and 22.6%, respectively, versus a national target of 60% for both. The percentage of adults receiving A1c testing at least twice a year was higher than the U.S. national target for 2010 for both men (69.0%) and women (65.7%) and for persons aged 18--64 years and those aged >65 years; however, the percentage was significantly lower in the 18--64 age group (65.5% versus 76.2%; p<0.05) (Table). The percentage who received annual foot examinations also was significantly lower among those aged 18--64 years than among those aged >65 years (43.8% versus 54.6%; p<0.05). However, for the other three preventive-care practices, no significant differences by age were observed. For all of the practices, the percentages for men and women were similar. Of the five preventive-care practices analyzed, 63.0% of adults with diabetes in Puerto Rico reported engaging in two or fewer practices, and 13.5% reported engaging in no preventive-care practices (Figure 2). A total of 37.0% of adults reported engaging in three or more practices, and 3.3% reported engaging in all five. Reported by: Z Kianes-Pérez, MS, M Pérez-Padua, L Pérez-Rivera, MPHE, Diabetes Prevention and Control Program, Puerto Rico Dept of Health. NR Burrows, MPH, RV Díaz-Kenney, MPH, LS Geiss, MA, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Effective interventions are available that can prevent or delay diabetes complications (1,2). Consistent with previous reports of diabetes-related preventive care in the United States (3--6), the findings in this report indicate that the percentages of adults with diabetes in Puerto Rico who engage in preventive-care practices, with the exception of A1c testing, were lower than U.S. national health targets for 2010. Fewer than 5% of adults with diabetes engaged in all five practices. Improvement in diabetes care, particularly in self-management education and in SMBG, is needed to achieve the U.S. national health objectives for 2010 and to reduce diabetes complications. In addition, younger persons with diabetes need interventions to improve their preventive care. The findings in this report are subject to at least three limitations. First, BRFSS collects data through telephone surveys that do not include institutionalized persons (e.g., nursing home residents) or persons without telephones. As a result, the percentages of persons with diabetes who engaged in preventive-care practices in this report might be higher than the actual percentages because persons without telephones are more likely to have lower levels of education and less likely to receive preventive care (3--6). Second, self-reported data are subject to recall bias, and the effect of this bias on the magnitude and direction of the results is unknown. Such bias might cause preventive-care practices to be either under- or overreported. Finally, BRFSS response rates in Puerto Rico ranged from 65.3% to 81.5% during the study period; however, compared with census data, BRFSS data have minimal bias (9). Since 1997, CDC has provided funding to the Diabetes Prevention and Control Program (DPCP) in Puerto Rico. DPCP adapted the Spanish version of CDC's train-the-trainer program, Diabetes Today (La Comunidad en Acción), to the Puerto Rican culture; the program is used to guide health professionals and community leaders in training lay health workers (promotores), improving diabetes self-management, and preventing diabetes complications. DPCP also develops protocols for standards of care and diabetes education materials, sponsors mass media and face-to-face educational campaigns focused on diabetes prevention and control, and collaborates with the Puerto Rico Diabetes Advisory Council and community-based organizations to improve diabetes care. DPCP implemented the Puerto Rico Diabetes Surveillance System by using data from the BRFSS diabetes module and information from health insurance companies on diabetes, its complications, and use of health-care services. The BRFSS diabetes module is also used to evaluate program objectives and activities. Continued surveillance is essential to monitor the effectiveness of measures to improve levels of preventive-care practices among persons with diabetes in Puerto Rico. References
* Hemoglobin A1c testing at least twice a year, 65% (objective 5-12†); annual dilated eye examination, 75% (objective 5-13); annual foot examination, 75% (objective 5-14); ever having education on diabetes self-management, 60% (objective 5-1); and self-monitoring of blood glucose at least once daily, 60% (objective 5-17). † Objective 5-12 was revised since its original publication. Figure 1 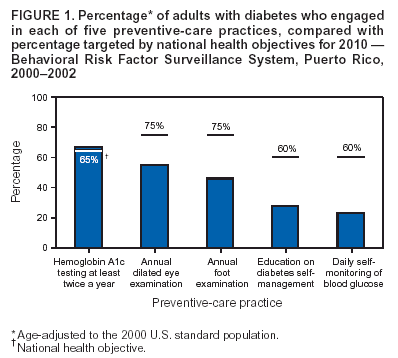 Return to top. Figure 2 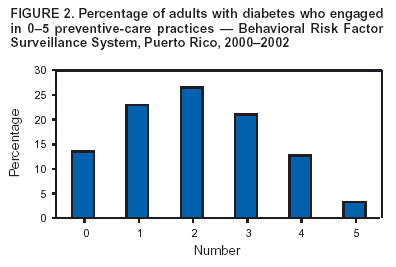 Return to top. Table 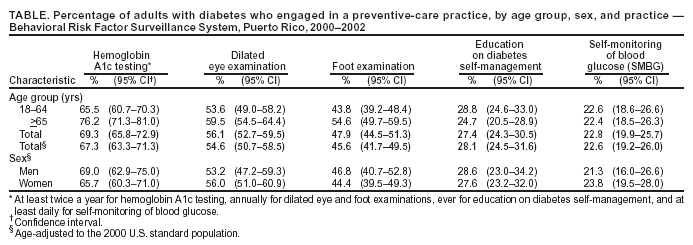 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/10/2004 |
|||||||||
This page last reviewed 11/10/2004
|