 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Violence-Related Behaviors Among High School Students --- United States, 1991--2003Homicide and suicide are responsible for approximately one fourth of deaths among persons aged 10--24 years in the United States (1). Two of the national health objectives for 2010 are to reduce the prevalence of physical fighting among adolescents to <32% and to reduce the prevalence of carrying a weapon by adolescents on school property to <4.9% (objective nos. 15-38 and 15-39) (2). To examine changes in violence-related behaviors among high school students in the United States during 1991--2003, CDC analyzed data from the national Youth Risk Behavior Survey (YRBS). This report summarizes the results of that analysis, which indicated that most violence-related behaviors decreased during 1991--2003; however, students increasingly were likely to miss school because they felt too unsafe to attend. In addition, in 2003, nearly one in 10 high school students reported being threatened or injured with a weapon on school property during the preceding 12 months. Schools and communities should continue efforts to establish physical and social environments that prevent violence and promote actual and perceived safety in schools. The national YRBS, a component of CDC's Youth Risk Behavior Surveillance System, used independent three-stage (i.e., primary sampling units, schools, and classes) cluster samples for the 1991--2003 surveys to obtain cross-sectional data representative of public- and private-school students in grades 9--12 in the 50 states and the District of Columbia. During 1991--2003, sample sizes ranged from 10,904 to 16,296, school response rates ranged from 70% to 81%, student response rates ranged from 83% to 90%, and overall response rates ranged from 60% to 70%. For each cross-sectional national survey, students completed an anonymous, self-administered questionnaire that included identically worded questions about violence. For this analysis, temporal changes during 1991--2003 for three behaviors were assessed: 1) weapon (e.g., a gun, knife, or club) carrying (on >1 of the 30 days preceding the survey), 2) physical fighting (one or more times during the 12 months preceding the survey), and 3) being in a physical fight that resulted in injuries that had to be treated by a doctor or nurse (one or more times during the 12 months preceding the survey). In addition, temporal changes from 1993--2003 for four school-related behaviors were assessed: 1) weapon carrying on school property (on >1 of the 30 days preceding the survey), 2) physical fighting on school property (one or more times during the 12 months preceding the survey), 3) being threatened or injured with a weapon on school property (one or more times during the 12 months preceding the survey), and 4) not going to school because of safety concerns (i.e., feeling too unsafe at school or on the way to or from school on >1 of the 30 days preceding the survey). Data are presented only for non-Hispanic black, non-Hispanic white, and Hispanic students because the numbers of students from other racial/ethnic populations were too small for meaningful analysis. Data were weighted to provide national estimates, and SUDAAN was used for all data analyses. Temporal changes were analyzed by using logistic regression analyses that assessed linear and quadratic time effects simultaneously and controlled for sex, race/ethnicity, and grade. Quadratic trends indicated significant but nonlinear trends in the data over time. When a significant quadratic trend accompanied a significant linear trend, the data demonstrated a nonlinear variation (e.g., leveling off or change in direction) in addition to an overall increase or decrease over time. All results were statistically significant (p<0.05) unless otherwise noted. Significant linear and quadratic trends were detected for weapon carrying. Overall, the prevalence of weapon carrying declined significantly, from 26.1% in 1991 to 18.3% in 1997, and then leveled off through 2003 (17.1%) (Table). Similar significant linear and quadratic trends were detected among female, male, white, 10th-, 11th-, and 12th-grade students. Among black, Hispanic, and 9th-grade students, a significant linear decline was detected during 1991--2003. Overall, physical fighting declined significantly, from 42.5% in 1991 to 33.0% in 2003. Physical fighting also declined significantly among all subgroups except 11th-grade students. Among 11th-grade students, physical fighting declined during 1991--1999 and then remained level through 2003. No significant changes were detected in the prevalence of being injured in a physical fight overall or by subgroup. Weapon carrying on school property declined significantly, from 11.8% in 1993 to 6.1% in 2003. Weapon carrying also declined significantly among female, male, white, Hispanic, 9th-, 10th-, and 11th-grade students. Significant linear and quadratic trends were detected for weapon carrying on school property among black and 12th-grade students, with the prevalence of carrying a weapon on school property declining during 1993--1999 and then remaining level through 2003. Physical fighting on school property declined significantly, from 16.2% in 1993 to 12.8% in 2003. A similar significant linear trend was detected among all subgroups. No significant changes were detected in the prevalence of being threatened or injured with a weapon on school property during 1993--2003 overall or among female, male, Hispanic, 10th-, and 12th-grade students. A significant linear increase during 1993--2003 was detected among white and 9th-grade students. Among black students, being threatened or injured with a weapon on school property declined during 1993--1999 and then increased through 2003. Among 11th-grade students, being threatened or injured with a weapon on school property declined during 1993--1999 and then remained level through 2003. Not going to school because of safety concerns increased significantly, from 4.4% in 1993 to 5.4% in 2003. Not going to school because of safety concerns also increased significantly among female, white, and 11th-grade students. No significant changes were detected during 1993--2003 among male, black, Hispanic, 9th-, 10th-, and 12th-grade students. Reported by: N Brener, PhD, R Lowry, MD, L Barrios, DrPH, Div of Adolescent and School Health, National Center for Chronic Disease Prevention and Health Promotion; T Simon, PhD, Div of Violence Prevention, National Center for Injury Prevention and Control; D Eaton, PhD, EIS Officer, CDC. Editorial Note:The declines observed in weapon carrying and physical fighting, both in general and on school property, correspond with a decline in the national youth homicide rate (3). However, not all violent behaviors among youths are declining. The prevalence of being injured in a physical fight has remained stable for each subgroup. In addition, the prevalence of being threatened or injured with a weapon on school property increased among white and 9th-grade students and increased in recent years among black students. The increasing prevalence of not going to school because of safety concerns might be attributed in part to the increases in students being threatened or injured with a weapon on school property as well as students' heightened sense of vulnerability after an increase in high-profile, school-associated, multiple-victim homicides during the 1990s (4,5). Efforts to establish physical and social environments that promote safety and prevent violence, such as those described in CDC's School Health Guidelines to Prevent Unintentional Injuries and Violence (6), are likely to reduce students' actual and perceived risk for violence. Prevention programs have been effective in helping young persons at high risk and their families acquire the knowledge, skills, and support needed to avoid violence (7,8). The findings in this report are subject to at least two limitations. First, these data pertain only to youths who attended high school. Nationwide, among persons aged 16--17 years, approximately 6% were not enrolled in a high school program and had not completed high school (9). Second, the extent of underreporting or overreporting in YRBS cannot be determined; however, the survey questions demonstrate test/retest reliability (10). Although the declines in violence-related behaviors are encouraging, prevention efforts must be sustained if the nation is to achieve its 2010 national health objectives. In 2003, one in three high school students reported involvement in a physical fight, and approximately one in 16 high school students reported carrying a weapon on school property. To further reduce violence-related behaviors among young persons and to have an impact on behaviors that are more resistant to change, continued efforts are needed to monitor these behaviors and to develop, evaluate, and disseminate effective prevention strategies. References
Table 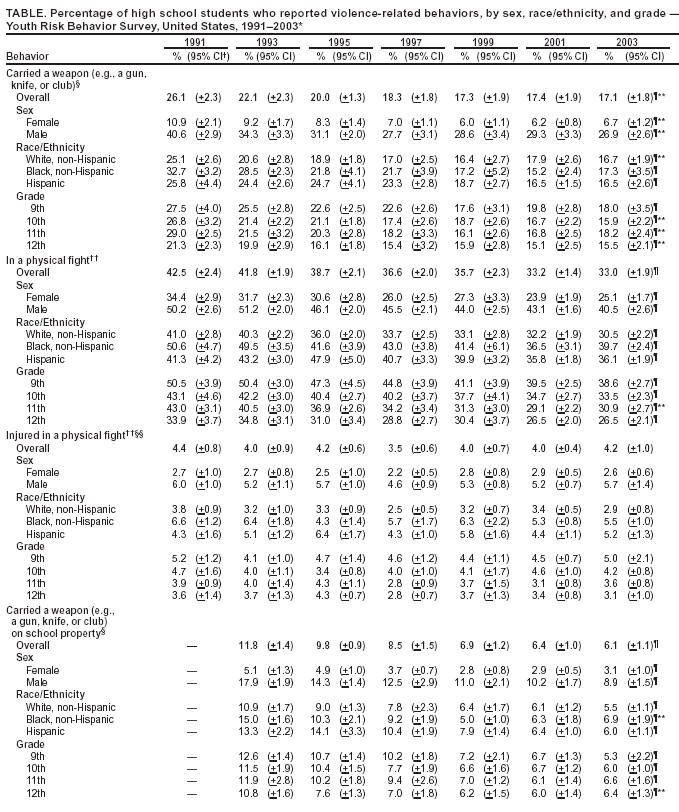 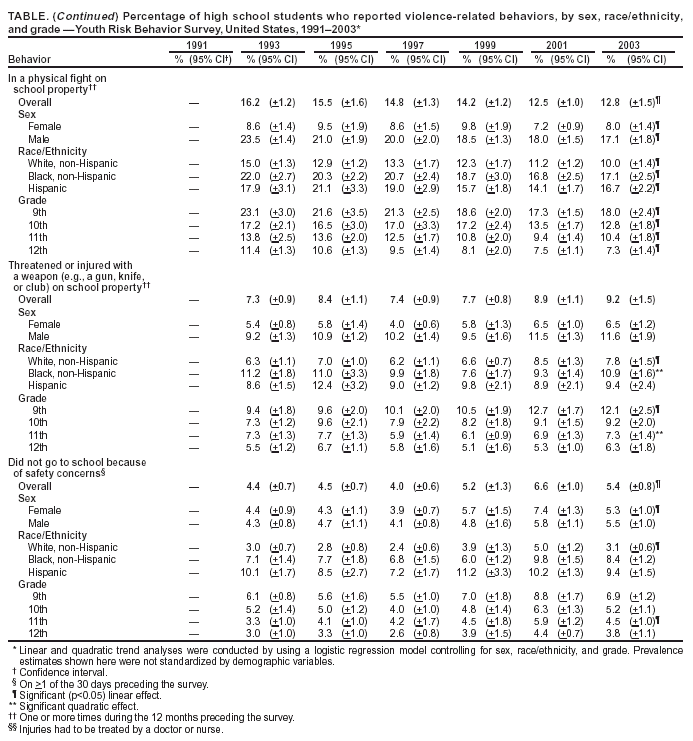 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/28/2004 |
|||||||||
This page last reviewed 7/28/2004
|