|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
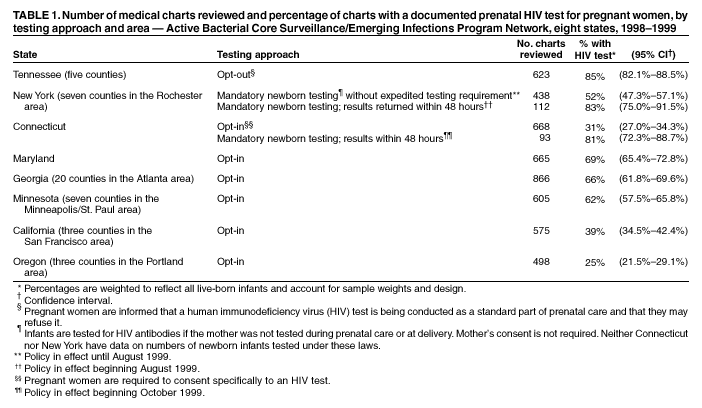
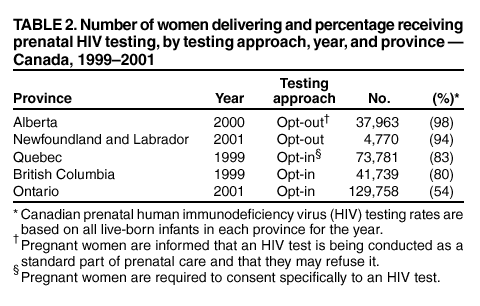
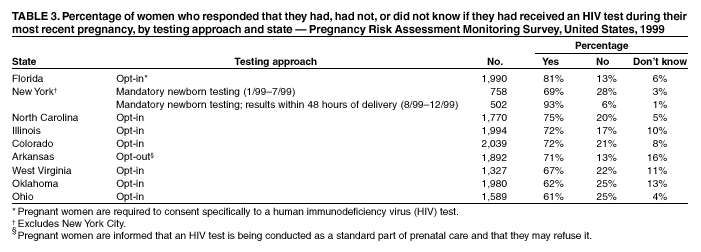
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. HIV Testing Among Pregnant Women --- United States and Canada, 1998--2001Since 1994, the availability of increasingly effective antiretroviral drugs for both the prevention of perinatal human immunodeficiency virus (HIV) transmission and maternal treatment has resulted in a greater emphasis on prenatal HIV testing and substantial increases in prenatal testing rates. In 2000, preliminary data indicated that 766 (93%) of 824 HIV-infected women in 25 states knew their HIV status before delivery (CDC, unpublished data, 2002). However, an estimated 280--370 perinatal HIV transmissions continue to occur in the United States each year (1). The primary strategy to prevent perinatal HIV transmission is to maximize prenatal HIV testing of pregnant women. States and Canadian provinces have implemented three different prenatal HIV-testing approaches. To assess their effectiveness, CDC reviewed prenatal HIV-antibody testing rates associated with these approaches. Medical record data suggest that the "opt-in" voluntary testing approach is associated with lower testing rates than either the "opt-out" voluntary testing approach or the mandatory newborn HIV testing approach. Under the opt-in approach, women typically are provided pre-HIV test counseling and must consent specifically to an HIV-antibody test. Under the opt-out approach, women are notified that an HIV test will be included in a standard battery of prenatal tests and procedures and that they may refuse testing (2). Under mandatory newborn HIV testing, newborns are tested for HIV, with or without the mother's consent, if the mother's HIV status is unknown at delivery. Three methods were used to estimate prenatal testing rates among all women who delivered, regardless of whether they received prenatal care. First, eight U.S. areas that participated during 1998--1999 in CDC's Active Bacterial Core Surveillance/Emerging Infections Program (ABC) Network assessed HIV testing during prenatal care and <2 days before delivery by reviewing a stratified random sample of labor and delivery records and prenatal records forwarded to birthing hospitals (3); in collaboration with CDC, network staff received a sample of records from all birthing hospitals in the surveillance areas and weighted testing rates to represent all live-born infants in those areas. Second, public health investigators in each of the five Canadian provinces tallied the number of HIV tests among pregnant women that were submitted to provincial laboratories and divided the total by an estimate of all live and stillborn births in each province during the same year. Third, CDC analyzed weighted data collected in 1999 by interviewers in nine states for CDC's Pregnancy Risk Assessment Monitoring System (PRAMS) (an ongoing, population-based survey conducted in 32 states and New York City among women who have given birth during the preceding 2--6 months [4]), who had asked women if they had been tested for HIV during pregnancy. Data on state prenatal HIV-testing policies were obtained from the American College of Obstetricians and Gynecologists (5). HIV-testing rates varied depending on which approach to testing was used. Rates for states using the opt-in approach to prenatal HIV testing included in the ABC Network ranged from 25% to 69% (Table 1), testing rates in Canada ranged from 54% to 83% (Table 2), and rates derived from PRAMS data ranged from 61% to 81% (Table 3). Two U.S. states (Arkansas and Tennessee) and two Canadian provinces (Alberta, and Newfoundland and Labrador) reported using an opt-out prenatal HIV-testing policy. ABC Network data indicated that Tennessee had a testing rate of 85% (Table 1). Canada's population-based data indicated a 98% testing rate in Alberta and a 94% testing rate in Newfoundland and Labrador (Table 2). PRAMS interview data indicated a 71% testing rate in Arkansas (Table 3), compared with a 57% testing rate early in 1997 before the law was implemented (Arkansas Department of Health, personal communication, 2002). Two states (New York and Connecticut) require HIV testing of newborns whose mothers were not tested during pregnancy. In New York, an ABC Network review of medical records in seven counties in the Rochester area indicated that the proportion of pregnant women who received a prenatal HIV test increased from 52% of 438 charts during January 1998--July 1999 to 83% of 112 charts during August--December 1999 after New York required that newborn HIV testing results be made available within 48 hours of specimen collection (Table 1). PRAMS data for 1999 indicated that the proportion of women statewide who reported having received an HIV test during pregnancy increased from 69% of 758 women during January--July to 93% of 502 during August--December (Table 3). In separate, statewide analyses of prenatal testing reported on newborn metabolic screening forms from all live-born infants, New York reported prenatal HIV-testing rates of 89% in 2000 and 93% in 2001 (New York State Department of Health, personal communication, 2002). In Connecticut, an ABC Network review of 668 charts indicated a testing rate of 31% during January 1998--September 1999, compared with 81% of 93 charts reviewed during October--December 1999 after enactment of the mandatory newborn testing law (Table 1). Reported by: A Roome, PhD, J Hadler MD, Connecticut Dept of Public Health. G Birkhead, MD, AIDS Institute, New York State Dept of Health. S King, MD, The Hospital for Sick Children, Toronto; C Archibald, MD, Health Canada. S Schrag, DPhil, Active Bacterial Core Surveillance/Emerging Infections Program Network, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; A Lansky, PhD, Pregnancy Risk Assessment Monitoring System, Div of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion; S Sansom, PhD, M Fowler, MD, I Onorato, MD, J Anderson, PhD, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:Prenatal HIV testing affords the best opportunity for the prevention of perinatal HIV transmission. On the basis of clinical trial data, perinatal HIV-transmission rates among HIV-infected women who begin antiretroviral treatment during pregnancy are as low as <2% (6), compared with 12%--13% early transmission rates among women who do not begin preventive treatment until labor and delivery or after birth (7) and 25% among women who receive no preventive treatment (8). Among the three prenatal HIV testing approaches assessed in this report, opt-out voluntary testing and the mandatory testing of newborns appear to be associated with the highest testing rates. On the basis of the chart-review methodology, prenatal testing rates were higher in Tennessee, which uses the opt-out approach, than rates in states using the opt-in approach and similar to rates achieved with mandatory newborn testing in New York during the same time period. A similar trend was observed among Canadian provinces. In New York and Connecticut, mandatory HIV testing of newborns was associated with increases in prenatal testing rates. On the basis of PRAMS data, three of seven states using the opt-in approach achieved lower prenatal HIV-testing rates than states using the opt-out or mandatory newborn testing approaches. Increases in prenatal HIV-testing rates were noted in states that shifted from an opt-in approach to either an opt-out or mandatory newborn testing approach and were probably associated with a greater likelihood that woman were offered HIV testing during prenatal care. Data from the Perinatal Guidelines Project indicated that the majority of women will accept HIV testing if it is recommended by their health-care provider (9). Perinatal HIV experts and professional organizations have advocated streamlining prenatal HIV pre-test counseling and consent procedures to reduce barriers to the offer of testing by health-care providers (1,2,10). The findings in this report are subject to at least seven limitations. First, testing results for each strategy are for all women, and the proportion of HIV-positive women who accepted testing under each strategy is not known. Second, among women who did not receive prenatal testing, the proportion of women who were not tested because they did not seek prenatal care is unknown. Third, among women who did not receive prenatal testing, the proportion of women who were tested at labor and delivery or whose infants were tested at birth is not known. Fourth, maternal self-reported data from PRAMS collected 2--6 months after delivery might be subject to recall bias. Fifth, PRAMS data do not indicate whether a prenatal-care provider was aware of the woman's HIV status. Sixth, among the women interviewed in PRAMS, up to 16% (in Arkansas) indicated they did not know if they had been tested. Finally, chart abstraction can document only prenatal HIV testing recorded in maternal medical records; without such documentation, clinicians might not be aware of the need to offer effective perinatal interventions to infected women and their HIV-exposed infants. This report emphasizes the need for better data to assess perinatal HIV testing rates in the United States. Ongoing, randomized reviews of prenatal, labor/delivery, and pediatric charts, with a sampling framework ensuring that the sample is representative of the population of women delivering, might provide the most valid approach to assessing a state's progress on perinatal HIV testing and prevention. CDC is working with states with high HIV prevalence rates among women of childbearing age and high numbers of pediatric AIDS cases to ensure standardized monitoring of prenatal testing rates. The data suggest that jurisdictions that use an opt-in approach and that have low prenatal HIV-testing rates should reevaluate their approach. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/14/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 11/14/2002