 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Unintentional Opiate Overdose Deaths --- King County, Washington, 1990--1999Heroin and other opiates are central nervous system depressants; in an opiate overdose, respiration slows, potentially resulting in hypoxia, coma, or death. In 1998, 140 deaths from unintentional opiate overdoses occurred in King County (which includes Seattle). To characterize these deaths, public health staff analyzed medical examiner data during 1990--1999. This report summarizes the results of that analysis, which indicate that the annual number of opiate overdoses increased 134% (from 47 to 110) and the county population increased 11.3% (1998 estimated population: 1.7 million) (1). Fatal unintentional opiate overdoses were defined as deaths that the King County medical examiner (KCME) determined to be the result of heroin or opiate intoxication of unintentional or unknown intent. Known and probable suicides were excluded from this analysis*. For this report, opiate overdose refers to overdoses of unintentional or unknown intent. KCME used observations at the death scene, autopsy findings, and toxicologic testing of body fluids to determine the cause of death†. The KCME database was searched for all deaths where heroin or opiate intoxication was listed on the death certificate as a primary, secondary, tertiary, or quaternary cause of death. Cases where opiates were detected, but overdose was not the primary cause of death, were excluded. Because a new software program was installed by KCME in 1995, detailed analyses were conducted on 1996--1999 data only; 1990--1995 data were used to calculate the annual number of deaths. Because the number of drug users in King County is unknown, the estimated county population (based on Washington State Office of Financial Management estimates for intercensal years 1998 and 1999 and U.S. Bureau of the Census figures for 1990) was used to calculate opiate overdose death rates. Standard errors of mortality rates and the statistical significance of the change in rates from 1990 to 1999 were computed, and PC-SAS was used for chi-square analysis of categorical data (2). The King County opiate overdose death rate increased from 3.1 per 100,000 population in 1990 to 6.6 in 1999, an increase of 112.9% (p<0.001). Opiate overdose deaths peaked in 1998, when there were 140 deaths and a death rate of 8.4 (Figure 1). During 1996--1999, 484 decedents ranged in age from 16 to 77 years (median: 40 years). Most overdose deaths were in men (84.7%) and whites (83.0%). Three fourths of overdose deaths occurred in Seattle, and 94% of all decedents were residents of King County. Of 110 opiate overdose deaths in King County in 1999, 84 (76.4%) deaths involved substances in addition to opiates (42, other drugs; 21, alcohol; and 21, alcohol and other drugs). For 98 (89.0%) decedents, direct evidence of injecting-drug use (e.g., injection marks or used syringes) was found at the overdose site. Since 1999, public health measures adopted by city and county government to address the increase in opiate overdose deaths in King County included authorizing a 50% increase in methadone treatment slots; improving access to methadone maintenance treatment with a motor-home--based clinic and through community-based agencies; providing preventive and limited substance-abuse treatment services in the local criminal justice system; increasing the availability of drug-free housing for persons in recovery; and providing education and interventions to children and adolescents to prevent initiation of drug use. The Seattle and King County governments have convened a task force on heroin use to develop new policies to improve access to substance-abuse treatment and extend prevention activities. A multidisciplinary, interagency working group composed of staff from Public Health--Seattle & King County, the Chemical Abuse and Dependency Services Division (King County Department of Community and Human Services), street outreach services, and providers of methadone treatment was established in January 2000 to plan an educational campaign targeting the user and substance-abuse treatment communities. In February, a Seattle hospital began dispensing methadone through a pharmacy for patients recovering from heroin addiction as part of a research project evaluating expanded access to methadone through primary-care physicians and pharmacies (3). Reported by: D Solet, PhD, Epidemiology, Planning and Evaluation Unit, H Hagan, PhD, Epidemiology Research Unit, J Nakagawara, MHA, Medical Examiner's Office, A Plough, PhD, Public Health--Seattle & King County, Seattle, Washington. JK Ball, PhD, Office of Applied Studies, Substance Abuse and Mental Health Svcs Administration. Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention; Office of Statistics and Programming, and Family and Intimate Violence Prevention Team, Div of Violence Prevention, National Center for Injury Prevention and Control; and an EIS Officer, CDC. Editorial Note:The findings in this report indicate that the opiate overdose death rate increased substantially in King County during 1990--1999. Although national figures on opiate overdose deaths were not available, opiate overdose deaths appear to be a problem in other U.S. cities as well. During 1994--1998, the Drug Abuse Warning Network (DAWN)§ received reports of 20,140 drug-induced deaths where opiates were detected. During 1994--1998, deaths reported to DAWN increased 25.7%. Heroin use has been increasing among injecting-drug users (IDUs) in a Seattle study since 1994 (4; H. Hagan, Public Health--Seattle & King County, personal communication, 1999). The proportion of new study recruits reporting heroin as their primary injection drug has been increasing, from 61% (n=655) in 1994 to 86% (n=524) in 1999 (5; H. Hagan, Public Health--Seattle & King County, personal communication, 2000). The risk for death during intravenous injection of an opiate is greater than from intramuscular or subcutaneous injection or from snorting or smoking because intravenous injection results in a more rapid rise in opiate levels in the blood (6). Most heroin used in King County is Mexican black tar, which is difficult to snort because of impurities and consistency. The purity of heroin available in King County has remained fairly stable since the early 1990s, ranging from 13.4% to 27.9% (Domestic Monitoring Program, Drug Enforcement Administration, unpublished data, 2000). In most opiate overdose deaths in King County, alcohol and other drugs were involved; these combinations can increase the likelihood of overdose (7). The findings in this report are subject to at least four limitations. First, the number of opiate overdose deaths was determined from a single data source. If opiate overdose deaths were not reported to or investigated by KCME, they were not included in the analysis, resulting in a possible underestimate of the overdose death rate. Second, the case definition includes "accidental" and "undetermined" overdose deaths; some of the undetermined deaths may have been suicides, resulting in a potential overestimate of the death rate. Third, nonresidents of King County were included in the analyses if they died in King County, possibly resulting in an overestimate of the death rate. Finally, if a family member or acquaintance was not available to provide information about the decedent's race or ethnicity, visual identification was used to assign race and ethnicity, potentially resulting in misclassification. Interventions to decrease unintentional opiate overdose deaths include preventing initiation of drug use and expanding substance-abuse treatment for addiction, particularly methadone maintenance. IDUs unable or unwilling to discontinue injecting should consider reducing heroin dose after illness or abstinence (e.g., because of incarceration); training in artificial respiration; and injecting in the presence of someone who can recognize an overdose, call emergency services, and administer artificial respiration if needed (8,9). Overdose prevention programs also must address IDUs' fear that calling for emergency assistance could result in arrest. Some programs train IDUs and their partners in the use of naloxone, an opiate antagonist highly effective in reversing the effects of opiate overdose but that can induce withdrawal symptoms and requires medical supervision (6). European programs that provide "safer injection room" facilities staffed by health-care workers have been associated with a decrease in drug overdose deaths (10). References
* From 1990 through 1999, an average of two opiate overdose suicides occurred per year (range: zero to five). † Opiates detected included heroin, morphine, fentanyl, hydrocodone, codeine, and methadone. Heroin rapidly metabolizes into morphine in the body; until mid-1999, when KCME tests began to differentiate between different types of morphine, heroin-related deaths were listed as morphine-related unless direct evidence of heroin use was found at the overdose site. § Managed by the Substance Abuse and Mental Health Services Administration, DAWN collects information on drug-abuse related deaths from participating medical examiners. The number of medical examiners participating in all years during 1994--1998 included 137 jurisdictions in 40 metropolitan areas. Figure 1 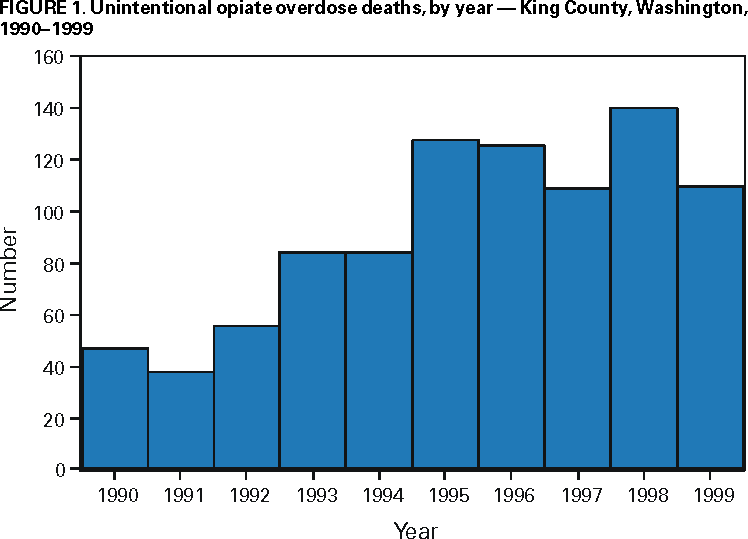 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/20/2000 |
|||||||||
This page last reviewed 5/2/01
|