 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Cigarette Smoking Among Secondary School Students --- Budapest, Hungary, 1995 and 1999The average per capita cigarette consumption in Hungary is among the highest in the world (World Health Organization [WHO], unpublished data, 1997) (1). In 1999, the Metropolitan Institute of State Public Health and Public Health Officer Service, Budapest, Hungary, collaborating with CDC, conducted a survey of cigarette smoking among secondary school students aged 14--18 years in Budapest (1999 population of Budapest: approximately 2 million), similar to a survey conducted in 1995 (2). This report summarizes the survey findings, which indicate that current smoking among secondary school students in Budapest increased from 36% in 1995 to 46% in 1999. The objective of the 1999 survey was to compare changes that had occurred since the 1995 survey in the prevalence of current* cigarette smoking, in the factors associated with current cigarette smoking, and in the smoking behaviors of current cigarette smokers (i.e., number of cigarettes smoked per day and number of days smoking occurred on school property). Among the 80,352 secondary school students in Budapest in 1999, 67,253 attended traditional high schools and 13,099 attended vocational/technical schools. Of 222 secondary schools (grades 9--12), 21 traditional high schools and nine vocational/technical schools were selected with a probability proportional to enrollment size. Classrooms in the 30 schools were selected randomly. All selected schools and classrooms agreed to participate, and all students in the selected classrooms were eligible to participate. From March through May 1999, 2615 (85%) of 3092 eligible students† completed a pretested, standardized questionnaire that included questions about tobacco use translated from the U.S. Youth Risk Behavior Survey (3). Of the 2615 completed surveys, 2434 (93%) were from students aged 14--18 years; 24 (<1.0%) were age 14 years, a number too small for meaningful analysis. Therefore, analysis of data from 1999 was limited to students aged 15--18 years. The 1995 data for students aged 15--18 years were compared with 1999 data using Epi Info version 6.0. Prevalence odds ratios (POR)§ and 95% confidence intervals (CIs) were calculated using CSAMPLE to account for the complex survey design (4). Among the 2410 students, 1148 (46.0%) (95% CI=42.4%--49.5%) reported current smoking (Table 1). Prevalence of current smoking among male and female students was similar (44.9% and 46.9%, respectively) (POR=0.9; 95% CI=0.8--1.1). Students aged 18 years were more likely to be current smokers than students aged 15 years (51.8% and 37.2%, respectively) (POR=1.8; 95% CI=1.3--2.6). Prevalence of current smoking was higher among vocational/technical students than traditional high school students (60.2% and 43.1%, respectively) (POR=2.0; 95% CI=1.5--2.6); among students whose friends smoked than those whose friends did not smoke (51.9% and 5.2%, respectively) (POR=19.5; 95% CI=9.8--38.9); among students who reported that they had seen a teacher smoking during the school year than those who had not seen a teacher smoking (47.2% and 35.8%, respectively) (POR=1.6; 95% CI=1.4--1.9); and among students with a family member who smoked than students whose family members did not smoke (51.9% and 36.6%, respectively) (POR=1.9; 95% CI=1.5--2.3). The prevalence of current smoking was similar among students who discussed issues related to smoking and health in any of their classes and those who did not receive such instruction (44.8% and 48.6%, respectively) (POR=0.9; 95% CI=0.7--1.1). Among students who were current smokers, 23.5% smoked >11 cigarettes on the days that they smoked, 46.7% smoked daily, and 36.9% smoked on school property on >10 days during the preceding month. From 1995 to 1999, current smoking increased among female students (35.2% versus 46.9%), 17-year-old students (39.4% versus 49.4%), 10th graders (32.8% versus 45.5%), and traditional high school students (31.5% versus 43.1%). Although the prevalence of daily smoking was similar among male and female students in 1999 (46.2% and 46.4%, respectively), daily smoking among female students increased from 32% in 1995 while the rate for male students remained stable. The percentage of secondary school students in Budapest who smoked >11 cigarettes per day during the preceding month increased from 1995 to 1999 (Table 2). Reported by: É Kiss, MD, Div of Health Promotion and Protection; F Ferenczi, E Végh, MD, Dept of Child and Youth Health, Div of Health Promotion and Protection; K Lun, MD, Metropolitan Institute of State Public Health and Public Health Officer Svc, Budapest, Republic of Hungary. Epidemiology Br, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion; and an EIS Officer, CDC. Editorial Note:The survey findings indicate that the prevalence of current cigarette smoking among secondary school students aged 15--18 years in Budapest increased significantly from 1995 to 1999. In 1999, the prevalence of current smoking among adolescents aged 15 years was 37.2%. This finding is consistent with smoking rates among adolescents aged 13--15 years during 1999 in the Russian Federation, Moscow, where 33.4% were current smokers (5). The estimated 46% smoking prevalence for students in Budapest in 1999 is higher than the estimated 28.4% prevalence for U.S. high school students (grades 9--12) who participated in the 1999 National Youth Tobacco Survey (6). In 1999, the Hungarian Parliament passed stronger legislation to enforce restrictions on smoking in the workplace and other public places. However, factors that may have contributed to the increased prevalence of smoking among youth in Budapest include a lack of regulation of the sale of cigarettes to minors until 1999 (T. Szilágyi, Health 21 Hungarian Foundation, personal communication, 2000), fewer advertising restrictions since 1997, free distribution of cigarette samples, weak health warnings, availability of contraband cigarettes, low fines for advertising violations, and lack of enforcement of existing regulations (1). The findings in this report are subject to at least one important limitation. These data apply only to youth who attended secondary school and are not representative of all persons in this age group (e.g., secondary school students who dropped out and approximately 80% of gypsy children who do not attend secondary school) (7). To better understand increasing prevalence rates of smoking among youth in Budapest and other central and eastern European countries, national health agencies must expand and evaluate tobacco prevention efforts and continue surveillance of trends in tobacco use among youth. The Global Youth Tobacco Survey (GYTS), sponsored by WHO's Tobacco Free Initiative (8) and CDC, will be conducted in Budapest by the end of 2000 and throughout Hungary in 2001. GYTS will evaluate a wide range of variables, including knowledge and attitudes about tobacco, exposure to environmental tobacco smoke, familiarity with prosmoking and antismoking media messages, and exposure to tobacco-use prevention curricula in schools. These efforts, along with Hungary's development of a plan for tobacco control as part of the Framework Convention on Tobacco Control (8), are important steps in curbing the increase in smoking among secondary school students in Hungary. References
* Smoked on at least 1 day during the 30 days preceding the survey. † 350 were absent; 127 refused to participate. § Used to calculate odds ratios from cross-sectional data; an odds ratio from studies of prevalent rather than incident cases. Table 1 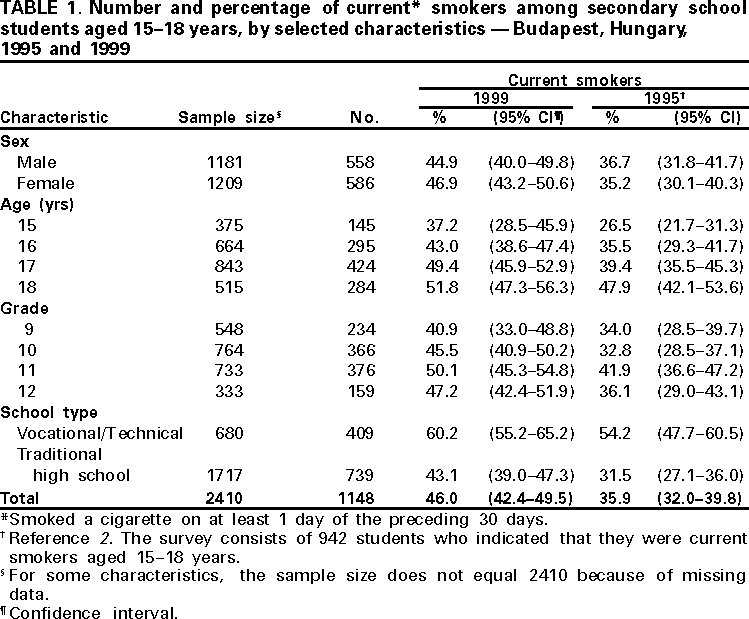 Return to top. Table 2 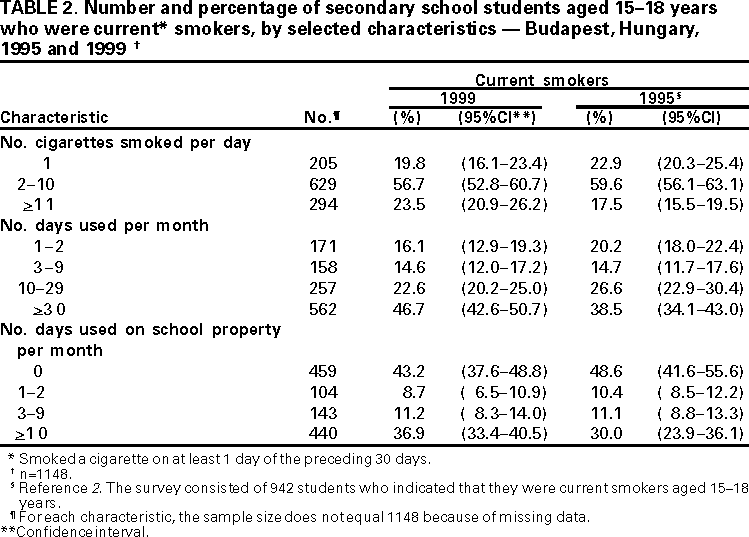 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/25/2000 |
|||||||||
This page last reviewed 5/2/01
|