 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Leisure-Time Physical Activity Among Overweight Adults ---United States, 1998In the United States, overweight and obesity have reached epidemic proportions among all segments of the population and regions of the country (1). Obesity is a risk factor for numerous chronic health conditions and weight loss can reduce risk factors for these conditions (2). National guidelines recommend that weight reduction should involve reducing calorie intake and increasing physical activity (3). The National Heart, Lung, and Blood Institute's clinical guidelines (3) and the federal dietary guidelines for Americans (4) recommend at least 30 minutes of physical activity on most days of the week for all healthy adults. To assess patterns of physical activity among overweight U.S. adults trying to lose weight, and to estimate the proportion who engage in leisure-time physical activity (LTPA) from selected demographic groups, CDC analyzed data from the 1998 Behavioral Risk Factor Surveillance System (BRFSS). This report summarizes the results of that analysis, which indicate that two thirds of overweight persons trying to lose weight reported using physical activity as a strategy for weight loss; however, only one fifth reported being active at recommended levels. BRFSS is a random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years. During 1998, 146,992 persons were surveyed in 50 states and the District of Columbia. Data on 11,953 (8.1%) persons were not eligible for this analysis because of pregnancy or missing information. Of those remaining, 72,624 (53.8%) were classified as overweight (body mass index [BMI]: 25.0--29.9) or obese (BMI: >30.0). For this analysis, the term overweight was used to describe persons who were overweight or obese. Of those overweight, 36,598 (50.4%) were trying to lose weight and were included in this analysis. The state median response rate for 1998 was 73.4%. Respondents who reported they were trying to lose weight were asked, "Are you using physical activity or exercise to lose weight?" Respondents also were asked to list their two most frequent LTPAs during the previous month and the frequency and duration of these activities. LTPA frequency was reported in times per week or per month. To calculate the national guidelines, for this analysis, it was assumed that LTPA occurred on a separate day. Prevalence estimates and 95% confidence intervals were calculated using SUDAAN (5). In 1998, 66.6% of overweight men and 62.2% of overweight women reported they were trying to lose weight by using physical activity (Table 1). For both sexes, using physical activity to lose weight was related inversely to age and BMI and directly related to education level. The prevalence of using physical activity to lose weight was highest among non-Hispanic black men and lowest among Hispanics of both sexes. The prevalence of using physical activity to lose weight was lowest among residents of southern states. In 1998, 62.7% of overweight adults using LTPA as a weight loss strategy participated in at least 30 minutes per session of LTPA, and 28.0% participated in LTPA five or more times per week. Among both sexes, walking was the most frequently reported activity (37.7% for men and 52.5% for women). Among men, running/jogging (10.7%), weight lifting (9.6%), and golfing (8.1%) were the most commonly reported activities; among women, aerobics (8.7%), gardening (8.2%), and using exercise machines (6.0%) were the most commonly reported activities (Figure 1). Reported by the following BRFSS coordinators: J Cook, MBA, Alabama; P Owen, Alaska; B Bender, MBA, Arizona; T Clark, Arkansas; B Davis, PhD, California; M Leff, MSPH, Colorado; M Adams, MPH, Connecticut; F Breukelman, Delaware; I Bullo, District of Columbia; S Hoecherl, Florida; L Martin, MS, Georgia; A Onaka, PhD, Hawaii; J Aydelotte, MA, Idaho; B Steiner, MS, Illinois; K Horvath, Indiana; K MacIntyre, Iowa; J Tasheff, Kansas; T Sparks, Kentucky; B Bates, MSPH, Louisiana; D Maines, Maine; A Weinstein, MA, Maryland; D Brooks, MPH, Massachusetts; H McGee, MPH, Michigan; N Salem, PhD, Minnesota; D Johnson, MS, Mississippi; T Murayi, PhD, Missouri; P Feigley, PhD, Montana; L Andelt, PhD, Nebraska; E DeJan, MPH, Nevada; L Powers, MA, New Hampshire; G Boeselager, MS, New Jersey; W Honey, MPH, New Mexico; C Baker, New York; P Buescher, PhD, North Carolina; L Shireley, MPH, North Dakota; P Pullen, Ohio; N Hann, MPH, Oklahoma; J Grant-Worley, MS, Oregon; L Mann, Pennsylvania; J Hesser, PhD, Rhode Island; M Wu, MD, South Carolina; M Gildemaster, South Dakota; D Ridings, Tennessee; K Condon, Texas; K Marti, Utah; C Roe, MS, Vermont; K Carswell, MPH, Virginia; K Wynkoop-Simmons, PhD, Washington; F King, West Virginia; P Imm, MS, Wisconsin; M Futa, MA, Wyoming. Behavioral Surveillance Br, Div of Adult and Community Health, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion; and an EIS Officer, CDC. Editorial Note:The findings in this report indicate that approximately two thirds of overweight adults trying to lose weight reported using physical activity to achieve weight reduction. However, only one fifth met the national recommendations for physical activity. Although most persons exercised >30 minutes per session, only a minority exercised at least five times a week. Therefore, low frequency of physical activity was the main reason the national guidelines for physical activity were not achieved. Walking was the preferred LTPA for both sexes; participation in other types of LTPAs varied by sex. The findings in this report are subject to at least two limitations. First, because weight was self-reported and overweight persons tend to underreport their weight (6), those classified as overweight probably represent a heavier subset of all overweight persons. Second, prevalences of LTPA levels are likely to be underestimated because a) respondents were allowed to report only two structured physical activities and b) estimates were based only on LTPAs; physical activity related to occupation could not be assessed. In comparison, prevalences of LTPA could be overestimated because BRFSS is a telephone survey and persons without telephones are likely to be less physically active than persons with telephones (7). Regular physical activity is a recognized factor for long-term weight maintenance (3). Increased physical activity boosts energy expenditure and reduces the risk for coronary heart disease beyond that produced by weight reduction alone (3). Increased physical activity can create a caloric deficit and contribute to weight loss. Although physical activity alone to achieve weight loss generally produces a 2%--3% decrease in body weight or BMI, increased physical activity is a useful adjunct to long-term weight loss (3). The finding that using physical activity as a method of weight loss was least common among obese, least educated, and older persons is concerning, but is consistent with previous findings (8). These patterns suggest that public health interventions to help these groups become physically active remain a challenge. Whether this disparity reflects a lack of knowledge about the value of physical activity in weight reduction, an inability to meet the recommended level of exercise, or poor motivation cannot be addressed with these data. Public health interventions that promote walking may be the most successful, because it is the most popular LTPA among overweight adults. In addition, walking is unique because of its safety, accessibility, and popularity among all groups (9,10). Strategies to promote walking may need to identify and address environmental barriers. Understanding sex-based differences in physical activity is important for tailoring interventions and counseling about weight-control practices. References
Table 1  Return to top. Figure 1 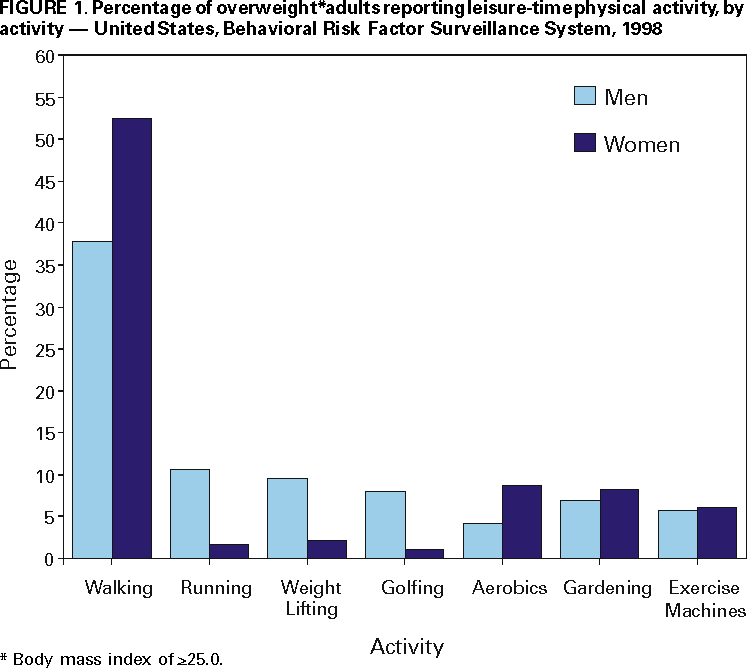 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 4/20/2000 |
|||||||||
This page last reviewed 5/2/01
|