 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
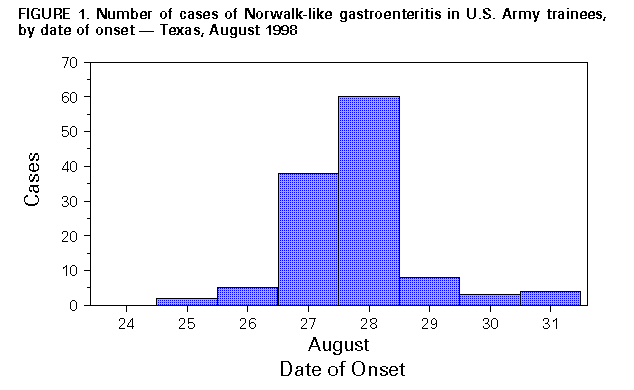
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Norwalk-Like Viral Gastroenteritis in U.S. Army Trainees -- Texas, 1998During August 27-September 1, 1998, 99 (12%) of 835 soldiers in one unit at a U.S. Army training center in El Paso, Texas, were hospitalized for acute gastroenteritis (AGE). Their symptoms included acute onset of vomiting, abdominal pain, diarrhea, and fever. Review of medical center admission records for AGE during the previous year indicated that fewer than five cases occurred each month. This report describes the outbreak investigation initiated on August 30 by a U.S. Army Epidemiologic Consultation Service (EPICON) team; the findings indicated the outbreak was caused by a Norwalk-like virus (NLV). The EPICON team reviewed data from the inpatient records of 90 ill soldiers. AGE was defined as three or more loose stools and/or vomiting within a 24-hour period in a soldier or employee at the training center during August 26-September 1. Illness was accompanied by a minimally elevated leukocyte count, mild thrombocytopenia, and low-grade fever. The median duration of hospitalization was 24 hours (range: 12-72 hours). Stool samples collected from persons with AGE on hospital admission were negative for bacterial and parasitic pathogens. Of 24 stool specimens sent to CDC for viral agent identification, 17 were positive by reverse transcriptase poly-merase chain reaction assays for NLVs (genogroup 2). Interviews with foodhandlers in the base's two dining facilities (DF1 and DF2) revealed illness in a confection baker, who had become ill in DF1 while baking crumb cake, pie, and rolls on August 26. One other DF1 employee who was not a foodhandler also reported self-limited gastrointestinal illness during August 27-29. No worker in DF2 reported illness. Cultures of food specimens from the ice cream dispenser in DF1 grew nonpathogenic coliform bacteria (Citrobacter diversus and Serratia liquefaciens); however, the sample was at room temperature before culture. Enterobacter cloacae coliform bacteria were cultured from the soda fountain in DF2. Water samples taken from multiple sites in the training compound and from elsewhere on post were all negative for coliform contamination. A questionnaire about food preferences, based on the previous week's menu, was administered to 86 hospitalized soldiers (84 of whom had eaten in DF1 during the 10 days before answering the questionnaire) and to 237 randomly selected soldiers from the training unit. Of the 237 nonhospitalized soldiers, 41 (17%) did not eat at DF1 during the 10 days before answering the questionnaire; 40 (17%) had illnesses that met the case definition. Thus, cases of AGE were characterized in 126 soldiers (Figure_1). To determine the point source of the outbreak, cases with onset during August 27-28 (n=98) were analyzed separately for odds ratios (ORs) of selected exposures (Table_1). The univariate OR for illness associated with dining at DF1 during the week before the outbreak was 9.8 (95% confidence interval=2.8-40.2). Two soldiers who ate exclusively at DF2 became ill, and one ill soldier reported not eating at either facility. Food items (crumb cake, pie, cinnamon rolls, and ice cream) and soda fountain dispensers were associated with illness by univariate analysis. Using multivariate analysis, only DF1 and the carbonated beverage dispensers remained strongly associated with illness (Table_1). Reported by: M Arness, MD, M Canham, MPH, B Feighner, MD, E Hoedebecke, DVM, J Cuthie, PhD, C Polyak, US Army Center for Health Promotion and Preventive Medicine, Edgewood, Maryland. DR Skillman, MD, J English, C Jenkins, T Barker, MD, William Beaumont Army Medical Center, El Paso, Texas. T Cieslak, MD, US Army Medical Research Institute of Infectious Diseases, Frederick, Maryland. DN Taylor, MD, Walter Reed Army Institute of Research, Washington, DC. Viral Gastroenterology Section and Infectious Disease Pathology Activity, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: NLVs, previously known as small round-structured viruses, are the most common cause of nonbacterial gastroenteritis outbreaks in adults (1,2). Classified in the family Caliciviridae (1,2), NLVs are transmitted by the fecal-oral route and have been implicated in 42%-71% of viral outbreaks associated with contaminated water and food since the Norwalk virus was identified (1,3,4). NLV outbreaks have been caused by eating contaminated raw shellfish and by unsanitary food preparation practices by foodhandlers (1,3-6). NLVs are hardy, ubiquitous, and extremely persistent in the environment, resisting disinfection and chlorination, and have caused serial gastroenteritis outbreaks (1,3,4). The epidemiologic evidence described in this report indicates that the outbreak was a point-source, propagated, foodborne viral illness. Although cases occurred before the onset of acute illness in the confection baker, he could have been the point source because he probably shed virus before the onset of clinical symptoms. The strong association with drinking carbonated beverages is not easily explained and may represent increased thirst among ill persons. The use of the Army hospital as a quarantine bay probably decreased secondary propagation of the illness. Prevention of future outbreaks of NLVs in U.S. military dining facilities or any food service establishment depends on vigilance and rigorous enforcement of simple measures to prevent food contamination. These measures include handwashing, exclusion of ill foodhandlers from the workplace, and basic hygiene and sanitation measures. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 03/25/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}