 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
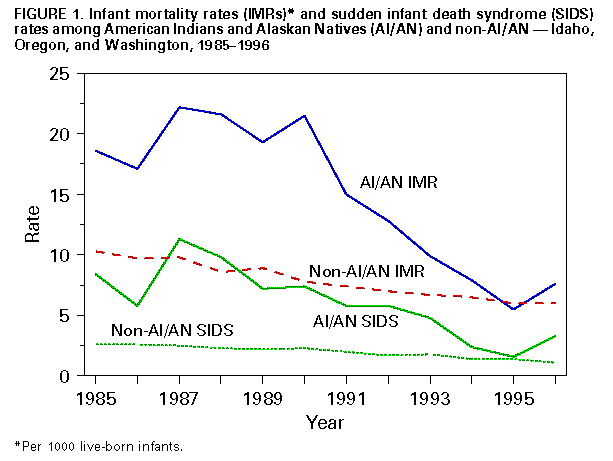
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Decrease in Infant Mortality and Sudden Infant Death Syndrome Among Northwest American Indians and Alaskan Natives -- Pacific Northwest, 1985-1996Although the infant mortality rate (IMR) has steadily declined in the United States since the early 1900s, the rate varies among racial/ethnic populations (1). A goal of the national health objectives for 2010 is to eliminate racial/ethnic health disparities (U.S. Department of Health and Human Services, unpublished data, 1999). Historically, IMRs among American Indians and Alaskan Natives (AI/AN) have been high (2). In addition, IMRs have varied among AI/AN populations (3). To determine recent trends in infant mortality among Northwest AI/AN, the Northwest Portland Area Indian Health Board (NPAIHB) analyzed annual IMRs among AI/AN in Idaho, Oregon, and Washington. In addition, because sudden infant death syndrome (SIDS) is the major contributor to excess infant mortality in Northwest AI/AN (4,5), NPAIHB analyzed SIDS rates to determine whether the decline in SIDS rates in the United States also was occurring among Northwest AI/AN. This report summarizes the results of this analysis and documents dramatic decreases in both SIDS and non-SIDS infant mortality. Annual vital statistics data for 1985-1996 were analyzed from the state health departments of Idaho, Oregon, and Washington and from CDC. Numerators for IMRs were all resident deaths for which the decedent was aged less than 365 days and for which the death certificate was linked to a birth certificate on which the race of the mother was AI/AN, regardless of whether the death occurred in the same calendar year as the birth. Denominators for IMRs were all resident live-born infants for each year for which the race of the mother on the birth certificate was AI/AN. Comparison rates for SIDS and overall infant mortality for all other races (non-AI/AN) were calculated by subtracting the AI/AN births and infant deaths annually for each state from the all-races totals obtained from CDC. Hispanic ethnicity was not considered in the analysis. Annual rate changes were compared with combined rates for 1985-1988, 1989-1992, and 1993-1996. These periods were selected for comparison because of the introduction in 1993 of several programmatic initiatives that might have influenced IMRs among Northwest AI/AN. Deaths attributed to SIDS were those for which the underlying cause of death was listed as International Classifications of Diseases, Ninth Revision, code 798.0. Statistical analysis was conducted using chi square tests for trends using EpiInfo (6). From 1985 through 1996, IMRs and SIDS rates decreased among Northwest AI/AN (Table_1). In particular, IMRs for Northwest AI/AN decreased from 20.0 per 1000 live-born infants during 1985-1988 to 7.7 during 1993-1996, a rate difference of 12.3 per 1000 population. During the same period, SIDS mortality rates decreased from 8.9 to 3.0, a rate difference of 5.9. Approximately half (48.0%) of the decline in AI/AN IMRs was attributable to the decline in SIDS. For the same three time periods, IMRs and SIDS rates also decreased for non-AI/AN in Idaho, Oregon, and Washington. For non-AI/AN, IMR declined from 9.6 during 1985-1988 to 6.3 during 1993-1996, a rate difference of 3.3, and the SIDS rate decreased from 2.5 to 1.4, a rate difference of 1.1. Approximately one third of the decrease in infant mortality in non-AI/AN resulted from the decline in SIDS. Annual SIDS rates and overall IMRs decreased substantially for both AI/AN and non-AI/AN during the study period (Figure_1). IMRs for Northwest AI/AN is approaching that for non-AI/AN in the same states. The small increase in deaths attributed to SIDS in 1996 did not differ significantly from the trend. Reported by: LD Robertson, MD, Northwest Portland Area Indian Health Board, Portland, Oregon. LA DeRoo, MPH, JA Gaudino, MD, Washington State Dept of Health. CG Hahn, MD, Idaho Dept of Health and Welfare. KD Rosenberg, MD, Oregon Health Div. Editorial NoteEditorial Note: The findings in this report document a dramatic decline in IMR among Northwest AI/AN during 1985-1996. Decreases in both SIDS and non-SIDS cases were observed across each of the last two time periods, but decreases were greatest during 1993-1996. The decline in SIDS among Northwest AI/AN is consistent with, but of a greater magnitude than, the substantial decreases in SIDS nationally that have been attributed to the success of the national Back to Sleep campaign (7). Multiple factors may have caused the decreases in SIDS and non-SIDS cases among Northwest AI/AN. Important risk factors that have been associated with SIDS include prone sleeping position and exposure to environmental tobacco smoke (ETS). In 1993, to reduce the risk for SIDS among Northwest AI/AN, the Portland Area Indian Health Service (IHS) (covering Idaho, Oregon, and Washington) initiated programs for parental education on nonprone infant sleep position and reduction of infant exposure to ETS. However, many Northwest AI/AN receive part or all of their health-care services outside the IHS health-care delivery system. As a result, the extent that Northwest AI/AN were exposed to these IHS programs is uncertain. As early as 1992, there was publicity in the Seattle area about increased risk for SIDS among infants sleeping prone, and in 1994 the national Back to Sleep program began. However, it is unknown whether there were substantial changes in the prevalence of prone sleeping position or exposure to ETS among Northwest AI/AN during the time periods. Factors that may have helped reduce non-SIDS IMRs among Northwest AI/AN include 1) structured activities by Portland area IHS programs initiated in 1993 to identify and manage high-risk pregnancies, 2) state programs such as the Washington State First Steps Medicaid expansion program for pregnant women and infants, 3) improved access to tertiary care for very low birth weight (less than 1500 g {less than 3 lbs, 3 oz}) newborns, and 4) improvements in technology (e.g., introduction of surfactant use in neonatal intensive-care units). The findings in this report are subject to at least four limitations. First, infant race was defined using the CDC's National Center for Health Statistics definition of race for infant mortality (i.e., for calculation of rates, the infant is assigned the mother's race), which differs from the IHS method (i.e., considering the race of the infant as AI/AN if either the mother or father is AI/AN); thus, these findings cannot be directly compared with published IHS data. Second, determining race for AI/AN from vital statistics data is problematic (8); however, using linked records as in this analysis can minimize this problem (9). Third, diagnostic shift could have occurred, resulting in infant deaths that formerly would have been attributed to SIDS being ascribed to other causes. However, this possibility has been examined recently in other populations (7) and was not found to be a substantial factor. Finally, a small number of infant death records could not be linked to a birth certificate and were excluded. More extensive analysis is needed to determine factors associated with the dramatic decreases in IMRs and SIDS rates among Northwest AI/AN. Further understanding of the protective factors would be useful for developing and implementing programs to reduce infant mortality in other AI/AN populations in which high rates of SIDS and non-SIDS cases have been documented (10). References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 03/11/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}