 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Elimination of Neonatal Tetanus -- Egypt, 1988-1994Neonatal tetanus (NT) is a leading cause of neonatal mortality in many parts of the world and, of vaccine-preventable diseases, is second only to measles worldwide as a cause of childhood mortality (1). In Egypt, although tetanus toxoid (TT) vaccination for pregnant women was introduced in 1973, a nationwide survey in 1986 estimated that the NT mortality risk was seven per 1000 live births (2); in 1987, only 9% of pregnant women received at least two doses of TT (TT2+) through the routine vaccination program. Consequently, in 1988, the Ministry of Health initiated an aggressive NT elimination program; this program included 1) annual nationwide TT vaccination campaigns during 1988-1993 targeting pregnant women, and 2) supplementary campaigns during 1992-1994 targeting all women of childbearing age in districts where NT rates were highest. This report describes efforts to eliminate NT in Egypt that resulted in an 85% decline in reported cases during 1988-1994. The annual nationwide TT vaccination campaigns from 1988 through 1993 targeted pregnant women in two rounds 1 month apart during November and December of each year. During each week-long campaign, mass media, community contacts, and mosque announcements were used in all 26 governorates of Egypt to increase public awareness of the need for TT vaccination during pregnancy. During these campaigns, nationwide TT2+ coverage increased from 9% in 1987 (before the vaccination campaigns began) to 73% in 1988 (the first year of the vaccination campaigns) (Figure_1). The increase in TT vaccination activity was sustained by the routine TT vaccination program throughout the year; the mean number of TT doses administered during noncampaign months increased from approximately 30,000 per month during 1987 and 1988 to 78,000 per month during 1989 and 1990. Reported NT cases declined from 6554 cases in 1988 to 3448 cases in 1989. Despite a sustained reduction in the national reported NT incidence from 3.7 cases per 1000 live births (LB) in 1987 to 1.6 cases per 1000 LB in 1991, the governorates with the highest reported NT incidence before the campaigns ( greater than 4 NT cases per 1000 LB) accounted for a disproportionate percentage of cases during 1988-1991 (Figure_2). For example, in 1991, 66% of NT cases were reported from eight governorates that contained only 32% of the total population. To improve coverage in these high-incidence governorates, the target population for both routine vaccination and the annual TT vaccination campaigns during 1992-1993 was expanded from pregnant women to include all married women of childbearing age in these governorates. Subsequently, the number of TT doses administered per campaign increased from an average of 485,000 doses in 1990 and 1991 (before the target group was expanded) to 873,000 doses in 1992 and 1993. Although the eight governorates reported 58% of the total NT cases in 1994, the reported incidence of NT was less than 1.5 cases per 1000 LB in all eight governorates and less than 1 case per 1000 LB in six governorates. Because of the difficulty in reaching the highest incidence populations with both routine TT vaccination services and vaccination campaigns, in 1992 a "high-risk" NT elimination strategy was introduced. High-risk districts in the 26 governorates * were those with an annual reported NT rate of greater than or equal to 1 case per 1000 LB; these districts were targeted for supplementary vaccination activities in addition to the annual TT vaccination campaigns. During 1992-1994, two rounds of TT vaccination were conducted 1 month apart using mobile teams, supplementary vaccination sites, and intensive news media promotion of vaccination to reach all women of childbearing age. The number of supplementary vaccination activities increased from 12 in 1992 to 24 in 1993 and to 40 in 1994. To improve assessment of the impact of the NT elimination program, ongoing efforts have been made to strengthen NT surveillance. In 1992, standardized NT case investigation forms and procedures were instituted nationwide, a daily telephonic notification system was introduced, and surveillance and vaccination data were analyzed at the national level by district. Even though surveillance was enhanced, the reported number of NT cases in Egypt decreased 63% from 2728 cases in 1991 (before the enhanced surveillance was established) (1.6 cases per 1000 LB) to 993 cases in 1994 (0.6 cases per 1000 LB). Similarly, the number of districts reporting greater than or equal to 1 NT cases per 1000 LB declined from 80 in 1992 (the first year for which district-level data were available) to 38 in 1994. Reported by: Child Survival Project, Ministry of Health, Cairo, Egypt. Regional Office for the Eastern Mediterranean Region, World Health Organization, Alexandria, Egypt. Expanded Program on Immunization, Global Program for Vaccines and Immunization, World Health Organization, Geneva, Switzerland. National Immunization Program, CDC. Editorial NoteEditorial Note: In 1994, an estimated 490,000 neonatal deaths worldwide were caused by NT **; however, 730,000 neonatal deaths were prevented in developing countries through vaccination of mothers with TT2+ or through clean delivery and cord-care practices (3). In 1989, the World Health Organization (WHO) adopted a resolution to eliminate NT worldwide (4), and in 1993 -- when the estimated global NT death rate was 6.5 cases per 1000 LB and global TT2+ coverage among pregnant women was 45% -- WHO defined the elimination of NT as a reduction in incidence to less than 1 case per 1000 LB in each health district of every country (1,5). To achieve and maintain NT elimination, greater than or equal to 80% of infants need to be protected at birth through vaccination of their mothers with TT2+ or through clean delivery and cord-care practices (4). In addition, effective surveillance is necessary to enable detection and timely investigation of cases. Efforts to eliminate NT in Egypt reflect the experiences of other countries with a high incidence of NT and illustrate options for improving these efforts (6). For example, the annual nationwide TT vaccination campaigns resulted in rapid increases in national TT2+ coverage, while improvements in surveillance indicated that NT cases were clustered in areas with limited access to clean childbirth and vaccination services. This persistent clustering of cases required targeted vaccination activities in high-risk districts to reach persons who consistently were missed by both routine vaccination services and the national TT campaigns. Efforts to provide supplementary TT vaccination at the district level have been implemented successfully in other countries (e.g., Indonesia and Thailand) (7,8). Because of the mortality caused by NT in developing countries and the difficulty in reaching "high risk" areas that are consistently missed by the routine TT vaccination program, specific strategies guided by surveillance data should be designed and implemented to reach those populations and geographic areas associated with the highest risks for NT. References
The total number of districts in Egypt were 214 in 1992, 218 in 1993, and 223 in 1994. ** Estimates of NT deaths are derived 1) from national mortality data, 2) from NT death rates from NT surveys, or 3) in the absence of surveys, by assuming that rates are similar for countries with similar socioeconomic conditions, then adjusting for TT coverage levels. Figure_1 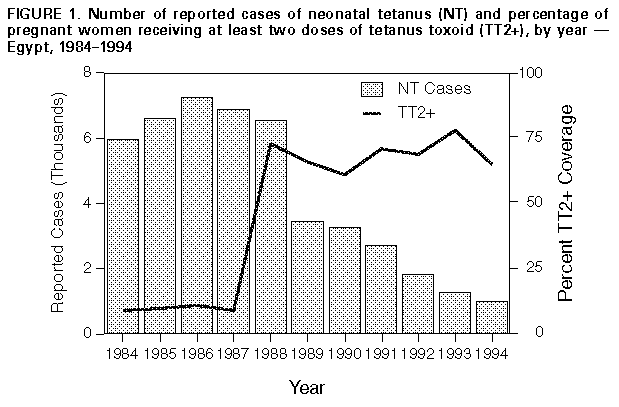 Return to top. Figure_2 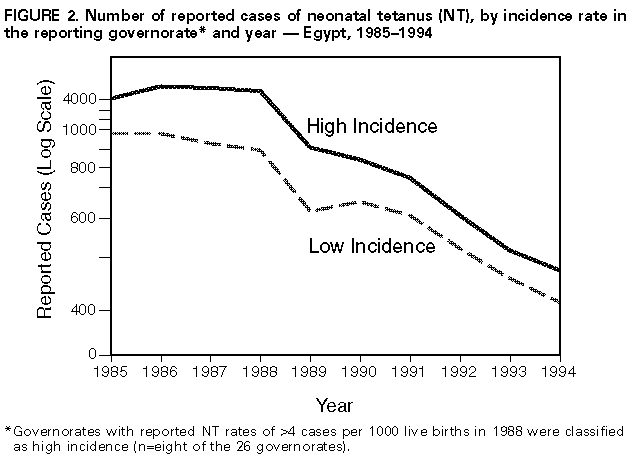 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}