 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Laboratory Practices for Diagnosis of Tuberculosis -- United States, 1994The increase in cases of tuberculosis (TB) during 1985-1992 and the emergence of multidrug-resistant Mycobacterium tuberculosis strains led to recommendations for rapid laboratory testing to support control efforts and selection of proper therapy (1,2). Many laboratories have adopted the recommendations to use rapid acid-fast bacilli (AFB) smears, growth detection (i.e., primary culture), identification, and drug-susceptibility testing for M. tuberculosis (3). The regulations implementing the 1988 Clinical Laboratory Improvement Amendments* (CLIA) require all laboratories that perform any mycobacteriology testing to enroll in federally approved proficiency testing (PT) programs. This report summarizes information reported by the laboratories to PT programs in the United States about their practices for M. tuberculosis. The PT programs submit samples of unknown content to laboratories for testing in the same manner as actual patient specimens; the laboratories subsequently report methods and test results to the program. In 1994, the U.S. Department of Health and Human Services approved six PT programs for mycobacteriology testing: five programs (the College of American Pathologists {CAP}; the states of New Jersey, New York, and Wisconsin; and the Commonwealth of Puerto Rico) provide PT testing for AFB smears, growth detection, organism identification, and drug-susceptibility testing; and one program (the American Association of Bioanalysts) provides testing for AFB smears only. To determine the number of laboratories that performed various levels of testing for M. tuberculosis, laboratories were classified into four categories based on the practices specifically reported for M. tuberculosis. These categories were laboratories that perform 1) AFB smears and refer all specimens for primary culture to another laboratory; 2) AFB smears and primary cultures for M. tuberculosis but refer all AFB-positive culture isolates for organism identification and drug-susceptibility tests; 3) AFB smears and primary culture with identification of M. tuberculosis isolates but refer isolates for drug-susceptibility testing; and 4) AFB smears, primary culture, identification, and drug-susceptibility testing for M. tuberculosis. Some laboratories must enroll in more than one PT program to meet the requirements of both state laboratory licensure programs and private laboratory accreditation programs. Therefore, because most laboratories were enrolled in the CAP PT program, the actual number of laboratories in each of the four categories ranges from a minimum that represents the enrollment of CAP only to a maximum that represents the total reported enrollment for all PT programs. In 1994, a total of 2862 mycobacteriology laboratories were enrolled in PT programs; 2459 (85%) were enrolled in CAP. Category-specific enrollment ranged from 506 (CAP only) to 683 (all PT programs) for laboratories that perform AFB smears only, 1126-1166 for those that perform primary culture without organism identification, 568-699 for those that perform primary culture and identification, and 259-314 for those that perform primary culture, identification, and drug-susceptibility testing Figure_1. Of the 2862 mycobacteriology laboratories, 2179 reported performing primary culture for M. tuberculosis. Of these, 1166 (54%) referred any AFB-positive isolates to another laboratory for organism identification and drug-susceptibility testing, 699 (32%) performed primary culture with identification, and 314 (14%) performed primary culture, identification, and drug-susceptibility testing. Similarly, of the 1953 laboratories enrolled in CAP only that reported performing primary culture for M. tuberculosis, 1126 (58%) referred any AFB-positive isolates to another laboratory for organism identification and drug-susceptibility testing, 568 (29%) performed primary culture with identification, and 259 (13%) performed primary culture, identification, and drug-susceptibility testing. Reported by: N Serafy, American Association of Bioanalysts, Brownsville, Texas. N Kubala, G Woods, MD, College of American Pathologists, Northfield, Illinois. M Salfinger, MD, I Salkin, PhD, New York State Dept of Health. R La Fisca, New Jersey Dept of Health. C Robles Rivera, Puerto Rico Dept of Health. N Bourdeau, Univ of Wisconsin Center for Health Sciences, Madison. Div of Laboratory Systems, Public Health Practice Program Office, CDC. Editorial NoteEditorial Note: Rapid laboratory testing to identify and determine the drug susceptibility of M. tuberculosis isolates is vital to effective diagnosis, treatment, and control of TB in the community. The findings in this report indicate that for a substantial proportion of TB cases, organism identification and drug-susceptibility determinations may be delayed because at least 54% of laboratories performing primary cultures for M. tuberculosis must refer AFB culture isolates to another laboratory for complete analysis. Although both solid and liquid media together are recommended for culturing M. tuberculosis, the liquid-culture method is needed to rapidly isolate and detect the organism in primary culture and to test susceptibility to the primary anti-TB drugs (1). In addition to decreasing the time required to detect and isolate mycobacteria, liquid-culture methods also increase the sensitivity of culture for M. tuberculosis (1,4). Although primary culture-isolation methods are not routinely reported to PT programs, a 1992 survey of 749 laboratories that performed primary culture with referral of all isolates to another laboratory indicated that 97 (13%) were using the recommended liquid-culture method (CAP, unpublished data, 1994). In addition, a survey of hospital laboratories in 1992 indicated that only 35 (14%) of 248 laboratories that referred isolates for identification of M. tuberculosis used the recommended liquid-culture method compared with 139 (50%) of 280 laboratories that routinely identified isolates of M. tuberculosis (CDC, unpublished data, 1994). Reasons for the continued use of solid-culture medium alone may reflect minimum test-volume requirements and higher costs associated with the liquid-culture system. The exclusive use of solid-medium culture methods delays isolation of M. tuberculosis by an average of 7-10 days (4), thereby delaying organism identification to confirm diagnosis. In addition, the referral of AFB-positive culture growth to another laboratory may result in delays associated with transport. These delays also may prolong determination of whether isolates are resistant to anti-TB drugs: in 1994, based on test results for 28 states, 8% of cases were resistant to isoniazid (INH) and 2% were resistant to both INH and rifampin (5). At least one state (i.e., New York) has regulations that prohibit laboratories from performing primary culture if the laboratory does not perform identification of M. tuberculosis. The findings in this report are subject to at least two limitations. First, data were unavailable about the proportion of all M. tuberculosis specimens tested by each of the four categories of laboratories enrolled in PT programs. Second, data were unavailable to determine whether laboratories that refer culture isolates for identification have adopted use of liquid-culture methods. Laboratories should select culture tests that provide rapid identification of M. tuberculosis and drug-susceptibility test results to enable early confirmation of the diagnosis and initiation of infection-control measures and case-finding. Laboratories that perform only primary culture for M. tuberculosis should determine whether referral of the patient specimen, rather than culture isolates, may decrease the time required for identification and drug-susceptibility testing. References
* 42 CFR 493.825. Figure_1 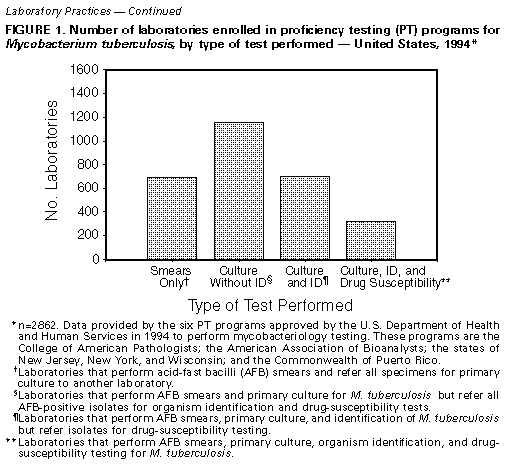 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}