 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Fatal and Nonfatal Suicide Attempts Among Adolescents -- Oregon, 1988-1993Suicide is the third leading cause of death among adolescents aged 15-19 years in the United States and second among adolescents in Oregon. During 1959-1961 and during 1990-1992, the rate of suicide in Oregon increased sixfold among 15-19-year-olds. During 1988-1991, the suicide rate for adolescents in Oregon (15.5 deaths per 100,000) was 39.6% higher than the U.S. rate (11.1). Because of the magnitude of this problem, in 1987 the state legislature in Oregon mandated that hospitals treating a child aged less than or equal to 17 years for injuries resulting from a suicide attempt report the attempt to the State Health Division, Oregon Department of Human Resources, and that the patient be referred for counseling; the Oregon Adolescent Suicide Attempt Data System (ASADS) was established in 1988. This report presents an analysis of data for adolescents aged less than or equal to 17 years from ASADS during 1988-1993. Notification of suicide attempt is made through a one-page report form, which is usually completed by emergency department or medical records personnel and is submitted monthly from all hospitals in the state. Hospitals use their own criteria to define attempts. Information collected includes age, race/ethnicity, sex, place of attempt, date of attempt, method of attempt, and whether the patient was admitted to the hospital. Beginning in 1990, data also were collected on reasons for the attempt and number of previous attempts. Data missing from attempt reports were imputed in proportion to known distributions for the specified variable. The proportion of missing data ranged from 0.1%-23.5%. In this analysis, fatal attempts were identified using death certificate data. During 1988-1993, a total of 3783 suicide attempts were reported for persons aged less than or equal to 17 years; of these, 3773 were by persons aged 10-17 years Table_1. Sex-specific attempt rates were 326.4 per 100,000 for females and 73.4 for males. Children as young as age 6 years had attempted suicide. The number of reported attempts increased steadily with age for males but peaked at age 15 years for females Figure_1. Characteristics of Fatal and Nonfatal Suicide Attempts During 1988-1993, most (2981 {78.8%}) suicide attempts were made in the residence of the attempter; 280 (7.4%), in another residence; 178 (4.7%), in school; and seven (0.2%), in jail. Attempts occurred more commonly during spring months (March, April, and May) (1106 {29.2%}) and least commonly during summer months (June, July, and August) (731 {19.3%}). In addition, attempts occurred most frequently on Mondays (660 {17.4%}) and least often on Saturdays (414 {11.0%}). Among youth aged 10-17 years, 123 (6.4 per 100,000) made a suicide attempt that resulted in death Table_1. The rate of fatal suicide attempts was three times greater for males (9.5) than for females (3.1). In addition, the proportion of attempts that were fatal was more than 100-fold higher among males (94 {11.5%}) than among females (29 {0.1%}). Although the risk for attempts was 3.8 times greater among youth aged 15-17 years than among those aged 10-14 years, the proportions of fatal attempts were similar among males and females in both age groups. During 1990-1993, of the 2511 persons who attempted suicide, 1042 (41.5%) reported having made at least one previous attempt during the preceding 5 years. Previous attempts occurred most often among those who indicated their reason for attempting suicide was rape/sexual abuse (149 {60.7%}), substance abuse (111 {56.6%}), or physical abuse (46 {54.0%}). Methods Used During 1988-1993, ingestion of drugs accounted for most (2857 {75.5%}) attempts Table_2; of the attempts involving drugs, analgesics accounted for 1354 (47.4%) (aspirin and acetaminophen were used most commonly). Cutting and piercing injuries accounted for 421 (11.1%) of the attempts, of which most were lacerations of the wrists. Most attempts by multiple methods were lacerations combined with a drug overdose. Drugs were used in 2440 (79.8%) attempts by females, compared with 417 (57.4%) by males Table_2. Males who attempted suicide were more likely than females to do so by suffocation/hanging, cutting/piercing, or use of firearms Table_2. Of all methods used to attempt suicide, those used most commonly were least likely to result in death (e.g., of attempts by drug overdose, 0.4% were fatal) Table_2. In comparison, 78.2% and 35.7% of attempts using firearms or poisonings with gas, respectively, were fatal. Of the 124 deaths among persons aged less than or equal to 17 years, most resulted from use of firearms (63.7%) or suffocation/hanging (18.5%). During 1990-1993, persons who had made multiple attempts were more likely to use suffocation/hanging (4.3%) and cutting/piercing (14.3%) than those making attempts for the first time (1.2% and 6.9%, respectively). Reasons for Suicide Attempt During 1990-1993, the most commonly reported reasons for attempting suicide were family discord (1492 {59.4%}), an argument with a boyfriend/girlfriend (819 {32.6%}), and school-related problems (578 {23.0%}) Table_3. A higher proportion of females (60.8%) and persons aged less than or equal to 12 years (73.0%) reported family discord as their reason for attempting suicide. Reported by: DD Hopkins, MS, JA Grant-Worley, MS, DW Fleming, MD, State Epidemiologist, State Health Div, Oregon Dept of Human Resources. National Center for Injury Prevention and Control, CDC. Editorial NoteEditorial Note: In Oregon, during 1988-1993, for every fatal suicide attempt by an adolescent, 31 nonfatal attempts were reported. Some attempts may not have been made with death as a goal but instead may have reflected a desire to resolve a difficult conflict, indicate an intolerable living situation, or elicit sympathy or guilt (1,2). Oregon is the only state with a legal requirement for reporting suicide attempts and a surveillance system for monitoring such attempts. The reported rate of suicide attempts among adolescents in Oregon during 1988-1993 based on ASADS data is substantially lower than previously reported using survey data. Based on the 1993 Youth Risk Behavior Survey, 2.7% of U.S. high school students reported making a suicide attempt during the previous 12 months that required medical attention (3); 3.2% (i.e., 3200 per 100,000) of Oregon high school students reported such attempts. Because ASADS is hospital-based and includes only attempts by persons who actually seek medical care, the findings may provide more valid information than other sources. For example, data from surveys often rely on the respondents' definition of attempted suicide, and only small proportions of respondents who report having attempted suicide actually have taken a substantive action to injure themselves (4). Furthermore, YRBS may overestimate the prevalence of suicide attempts among high school students. However, ADADS probably underestimates the occurrence of suicide attempts in Oregon for at least four reasons. First, hospital reporting may be incomplete; in addition, reporting hospitals may use different criteria in determining whether a patient attempted suicide. Second, reports of adolescent suicide attempts are not required from clinics or physicians' offices; some attempters may have been treated in these settings, especially those living in rural areas. Third, attempts by adolescents who did not require professional medical care were not reported. Finally, when persons from Oregon receive treatment in another state for a suicide attempt, the event is unreported. In Oregon, firearms were used most often in fatal suicide attempts, and most attempts involving firearms were fatal. Nationally, 81% of the increase in suicide among persons aged 15-19 years during 1980-1992 was related to use of firearms (5). Controlling access to firearms is an important prevention measure; however, storing weapons unloaded and locked may not prevent intentionally inflicted gunshot wounds among suicidal youth (6). Because an attempt with a gun usually results in death, parents and other persons who have responsibility for children should ensure that at-risk adolescents have no access to guns. ASADS represents an initial effort to examine the magnitude and epidemiology of intentionally self-inflicted injury among adolescents. This surveillance system was the first statewide system established to quantify the incidence of adolescent suicide attempts and to characterize the attempts and attempters. Although the system still must undergo vigorous evaluation (7), it provides essential information that will be useful in applying public health measures to the problem of suicide (8). Data from ASADS are being used to develop public and private suicide-education programs. For example, the Oregon Health Division has formed a task force to review the data and propose intervention methods. This approach may be adopted for use in other states to permit characterization of persons attempting suicide and to assist in refining prevention and early-intervention measures. References
Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Number and rate * of fatal and nonfatal suicide attempts among persons aged
10-17 years, by age group and sex -- Oregon, 1988-1993
======================================================================================
Male Female Total
Attempt/ ----------- ------------ ------------
Age group No. Rate No. Rate No. Rate
-------------------------------------------------------------
Nonfatal +
10-14 yrs 167 26.6 1037 174.0 1204 98.4
15-17 yrs 556 156.1 2013 594.4 2569 369.7
Total 723 73.4 3050 326.4 3773 196.6
Fatal &
10-14 yrs 22 3. 5 10 1.7 32 2.6
15-17 yrs 72 20.2 19 5.6 91 13.1
Total 94 9.5 29 3.1 123 6.4
-------------------------------------------------------------
* Per 100,000 population in specified group.
+ Source: Oregon Adolescent Suicide Attempt Data System.
& Source: Oregon death certificate data.
======================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Percentage of fatal and nonfatal suicide attempts among persons aged <= 17 years, by sex, age group, and method
used -- Oregon, 1988-1993
===============================================================================================================================
Nonfatal attempts *
------------------------------------------------------------------------
Sex (%) Age group (yrs) (%)
Total attempts ------------------ ---------------------------- % Fatal % Attempts
---------------- Male Female <= 12 13-14 15-17 Attempts + resulting in
Method No. (%) (n=726) (n=3057) (n=182) (n=1029) (n=2572) (n=124) death &
-----------------------------------------------------------------------------------------------------------------------------
Poisoning, drugs 2857 ( 75.5) 57.4 79.8 75.3 77.5 74.8 9.7 0.4
Poisoning, solids
and liquids 174 ( 4.6) 6.6 4.0 6.0 5.5 4.1 0.8 0.6
Poisoning, gas 8 ( 0.2) 1.0 0.1 0 0.3 0.2 4.0 35.7
Suffocation/Hanging 91 ( 2.4) 7.0 1.3 8.2 2.1 2.1 18.5 20.2
Drowning 4 ( 0.1) 0.4 0.1 0 0.1 0.2 -- --
Using firearms 23 ( 0.6) 2.6 0.2 0 0.6 0.8 63.7 78.2
Cutting/Piercing 421 ( 11.1) 16.3 9.9 7.1 9.9 11.9 -- --
Jumping from a
high place 23 ( 0.6) 1.7 0.3 -- 0.5 0.7 -- --
Other @ 182 ( 4.8) 7.0 4.2 3.3 3.6 5.3 3.2 2.2
Total 3783 (100.0) 100.0 100.0 100.0 100.0 100.0 100.0 3.2
-----------------------------------------------------------------------------------------------------------------------------
* Source: Oregon Adolescent Suicide Attempt Data System.
+ Source: Oregon death certificate data.
& Calculated by dividing the number of fatal attempts in a category by the total number of attempts in that category.
@ Includes attempts by multiple methods.
===============================================================================================================================
Return to top. Table_3 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 3. Percentage of persons aged <= 17 years who reported reasons for attempting
suicide, * by age and sex -- Oregon, 1990-1993 +
===================================================================================================
Sex Age group (yrs)
----------------- --------------------------
Male Female <= 12 13-14 15-17 Total &
Reason (n=436) (n=1749) (n=100) (n=640) (n=1490) (n=2231)
------------------------------------------------------------------------------------------
Family discord 53.9 60.8 73.0 65.0 56.1 59.4
Argument with
boyfriend/girlfriend 31.0 33.0 8.0 23.1 38.3 32.6
School-related problems 27.5 21.9 32.0 26.9 20.7 23.0
Rape/sexual abuse 4.1 11.2 7.0 13.0 8.7 9.8
Peer pressure/conflict 7.3 8.2 10.0 10.0 7.0 8.0
Substance abuse 15.1 6.0 3.0 5.9 8.9 7.8
Move or new school 5.7 6.0 7.0 8.6 4.8 6.0
Legal system encounters 14.0 2.6 4.0 4.7 5.0 4.8
Death of family
member/friend 4.8 4.5 6.0 4.2 4.6 4.5
Physical abuse 3.7 3.3 5.0 2.7 3.6 3.4
Suicide of friend/relative @ 4.4 3.1 2.0 4.8 2.8 3.4
Pregnancy 0.9 2.7 -- 1.6 2.9 2.4
Other reasons 15.8 14.1 9.0 13.9 15.0 14.4
------------------------------------------------------------------------------------------
* Categories are not mutually exclusive because more than one reason may have been reported.
+ Source: Oregon Adolescent Suicide Attempt Data System. 1990 was the first full year the
reason for the attempt was collected. Only attempts for which reasons were given are included.
& Includes one person for whom sex and age data were missing.
@ Includes suicide attempts.
==================================================================================================
Return to top. Figure_1 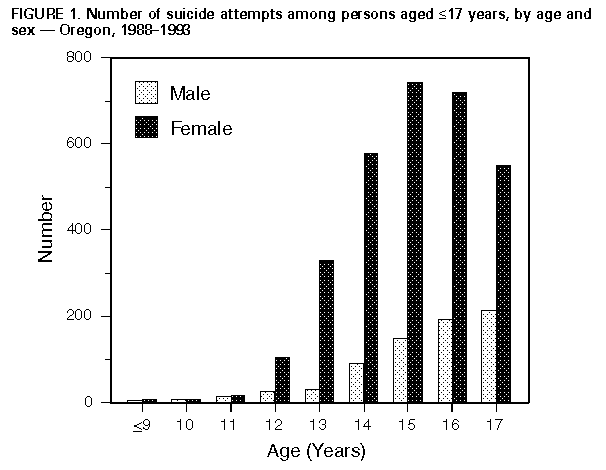 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}