 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
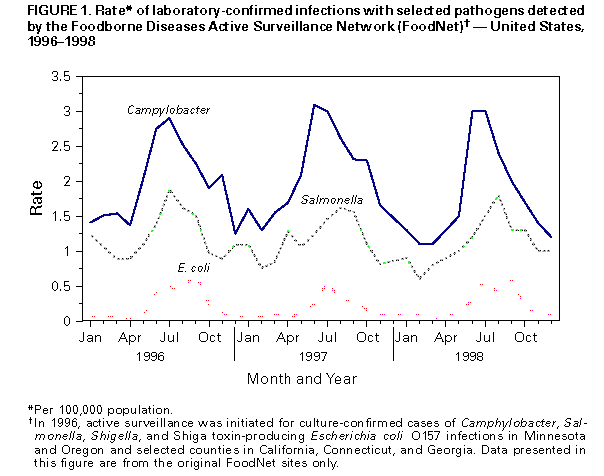
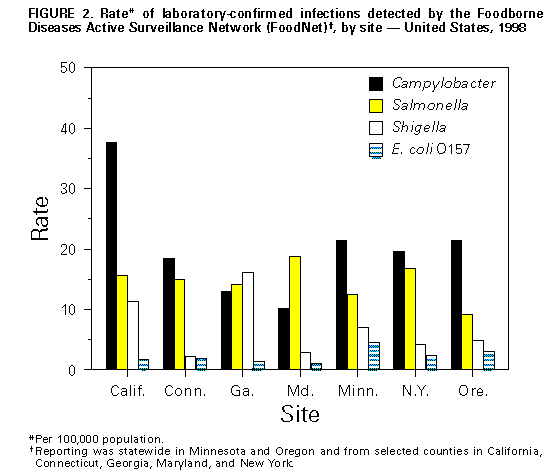
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Incidence of Foodborne Illnesses: Preliminary Data from the Foodborne Diseases Active Surveillance Network (FoodNet) -- United States, 1998Estimates of the magnitude of foodborne illness in the United States have been imprecise. To quantify, better understand, and more precisely monitor foodborne illness, since 1996 the Foodborne Diseases Active Surveillance Network (FoodNet) has collected data to monitor nine foodborne diseases in selected U.S. sites (1). This report describes preliminary data from FoodNet surveillance for 1998 and compares findings with those for 1996 and 1997; compared with 1996, the overall incidence of the foodborne illnesses under surveillance during 1998 declined, particularly for salmonellosis and campylobacteriosis, and the data continued to demonstrate regional and seasonal differences in the reported incidence of diseases. In 1996, active surveillance was initiated for culture-confirmed cases of Campylobacter, Shiga toxin-producing Escherichia coli O157, Listeria, Salmonella, Shigella, Vibrio, and Yersinia infections in Minnesota and Oregon and in selected counties in California, Connecticut, and Georgia. In 1997, surveillance for laboratory-confirmed cases of Cryptosporidium and Cyclospora infections were added. In 1998, active surveillance for these nine pathogens was initiated in selected counties in Maryland and New York. To identify cases, surveillance personnel contacted each clinical laboratory in their catchment areas either weekly or monthly, depending on the size of the clinical laboratory. Preliminary annual incidence was calculated using the number of cases reported by those laboratories for 1998 as the numerator and 1997 population estimates as the denominator (2); final incidence will be available once 1998 population estimates are available in mid-1999. All the rates contained in this article are considered preliminary. Monthly incidence was calculated based on date of specimen collection. 1998 Surveillance During 1998, 9787 laboratory-confirmed cases of nine diseases under surveillance were identified: 4031 of campylobacteriosis, 2849 of salmonellosis, 1483 of shigellosis, 565 of cryptosporidiosis, 508 of E. coli O157 infections, 186 of yersiniosis, 106 of listeriosis, 50 of Vibrio infections, and nine of cyclosporiasis. Among the 2670 Salmonella isolates serotyped, 808 (30%) were serotype Typhimurium, 406 (15%) were serotype Enteritidis (SE), and 168 (6%) were serotype Heidelberg; 179 (6%) were untyped. Isolation rates varied by season for several pathogens: 46% of E. coli O157, 41% of Campylobacter, and 35% of Salmonella were isolated during June-August (Figure_1). Fifty percent of cyclosporiasis cases and 33% of cryptosporidiosis cases were identified during June-August. Yersiniosis was more likely to occur during winter months, with 41% of cases reported in January, February, or December. Listeria, not usually tested for in stool, was isolated from normally sterile sites, including blood and cerebrospinal fluid, in 93% of reported listeriosis cases. In 8% of yersiniosis cases, 7% of salmonellosis cases, and less than or equal to 1% of shigellosis and campylobacteriosis cases, the organism was isolated from normally sterile sites. For all reporting sites, incidence was highest for campylobacteriosis (19.7 per 100,000 population), salmonellosis (13.9) and shigellosis (7.2). Substantial variation in incidence was observed among the sites for some pathogens (Figure_2). The incidence of campylobacteriosis ranged from 10.2 in Maryland to 37.7 in California. Although overall salmonellosis incidence was similar among the sites, the rates for infections with specific Salmonella serotypes varied; rates of infection with SE ranged from 0.7 in Georgia and New York to 5.1 in Maryland. Rates of infection with Typhimurium ranged from 3.1 in California and New York to 5.2 in Maryland. Shigellosis incidence ranged from 2.2 in Connecticut to 16.0 in Georgia. Incidence of E. coli O157 infections ranged from 1.1 in Maryland to 4.5 in Minnesota, and for yersiniosis ranged from 0.4 in New York to 1.6 in California and Georgia. The incidence of cryptosporidiosis ranged from 0.6 in Maryland to 3.7 in Minnesota. Comparison of Preliminary 1998 Data with 1996 and 1997 Data Comparing data from the five original FoodNet sites, overall incidence of laboratory-confirmed infections caused by the pathogens under surveillance declined from 1996 to 1998 (Table_1). Over this 3-year period, the largest decrease in bacterial pathogen-specific rates occurred in cases of infection caused by Salmonella (14.5 in 1996 to 12.4 in 1998, a 14% decline). This decrease was particularly pronounced for SE, which decreased 44% (from 2.5 to 1.4). Campylobacteriosis rates increased 7% from 1996 to 1997 and then decreased 14% (from 25.2 to 21.7) from 1997 to 1998. After declining 15% from 1996 to 1997, rates of E. coli O157 infection increased 22% from 1997 to 1998 (from 2.3 to 2.8). Similarly, the incidence of shigellosis decreased 16% from 1996 to 1997, but increased 13% from 1997 to 1998 (from 7.5 to 8.5). The incidence of infections caused by Vibrio, which increased from 1996 to 1997, remained elevated in 1998. The incidence of listeriosis and yersiniosis remained essentially unchanged during the 3-year period. Comparing the data on parasitic diseases from 1997 to 1998 (using only the sites reporting in both years), decreases occurred in the incidence of illness caused by Cryptosporidium, which decreased 7% (from 2.7 to 2.5), and by Cyclospora, which decreased from 0.3 to 0. In 1998 compared with 1997, Georgia reported a slight overall increase in the combined incidence of illnesses caused by the seven bacterial pathogens under surveillance; California, Connecticut, Minnesota, and Oregon reported decreases. Reported by: S Shallow, MPH, M Samuel, DrPH, A McNees, MPH, G Rothrock, MPH, California Emerging Infections Program, D Vugia, MD, S Waterman, MD, State Epidemiologist, California Dept of Health Svcs. T Fiorentino, MPH, R Marcus, MPH, G Kazi, MPH, School of Medicine, Yale Univ, New Haven; P Mshar, M Cartter, MD, J Hadler, MD, State Epidemiologist, Connecticut State Dept of Public Health. M Farley, MD, M Bardsley, MPH, S Segler, MPH, Emory Univ School of Medicine; J Koehler, DVM, P Blake, MD, K Toomey, MD, State Epidemiologist, Div of Public Health, Georgia Dept of Human Resources. M Pass, Johns Hopkins Univ School of Hygiene and Public Health, Baltimore; Y Wong Univ of Maryland Hospital, Baltimore; K Henning, L Gay, M Carter, D Dwyer, MD, State Epidemiologist, Maryland Dept of Health and Mental Hygiene. J Wicklund, MPH, C Hedberg, PhD, M Osterholm, PhD, State Epidemiologist, Minnesota Dept of Public Health. S Zanski, D Morse, MD, New York State Dept of Health. M Cassidy, T McGivern, R Stanton, B Shiferaw, MD, P Cieslak, MD, D Fleming, MD, State Epidemiologist, Oregon Health Div. Office of Public Health and Science, Food Safety and Inspection Svc, US Dept of Agriculture. Center for Food Safety and Applied Nutrition, Food and Drug Administration. Foodborne and Diarrheal Diseases Br, Div of Bacterial and Mycotic Diseases; Epidemiology Br, Div of Parasitic Diseases; and Office of the Director, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Each year, millions of persons experience foodborne illness, though only a fraction seek medical care and an even smaller number submit laboratory specimens. FoodNet provides a precise measure of the laboratory-diagnosed cases of specific foodborne illnesses and performs additional surveys and studies to interpret trends over time. The 1998 FoodNet data indicate a decline in several of the major bacterial and parasitic causes of foodborne illness. These declines might in part reflect annual fluctuations in the incidence of foodborne illnesses and temporal variations in diagnostic practices. The trends also may reflect implementation of disease prevention efforts. The declines in salmonellosis and campylobacteriosis may reflect changes in meat and poultry processing plants in the United States mandated by the Pathogen Reduction and Hazard Analysis and Critical Control Points (HACCP) rule of the U.S. Department of Agriculture (USDA). HACCP consists of production process controls, standard sanitation procedures, and microbial testing (by both food-processing plants and USDA) designed to reduce foodborne illnesses by monitoring and decreasing microbial contamination in food processing plants. HACCP was implemented by the largest producers in the food industry in January 1998. The decline from 1996 to 1998 in the incidence of salmonellosis parallels the reported decline in the percentage of meat and poultry products tested at large, federally inspected processing plants that were positive for Salmonella (3). Reasons for the decline in SE isolates remain under investigation. SE commonly has been associated with eating undercooked eggs (4), particularly in outbreaks. Implementation of an egg quality-assurance program with microbiologic testing and egg diversion (5) in some states may have contributed to the decline in reported cases of human illness caused by SE. This decline also might in part be explained by the decrease in the percentage of poultry products testing positive for Salmonella in large processing plants; recent evidence suggests that poultry meat might be a source of sporadic SE infections (6). Other changes in rates of foodborne illness may be explained by known events. For example, the large reduction in cyclosporiasis follows restrictions on the import of raspberries into the United States after a large outbreak was traced to this food (7). The continued elevation in reported rates of Vibrio infections reflects several multi-state outbreaks of V. parahaemolyticus in 1997 and 1998 (8,9). However, the reasons for the changes in the incidence E. coli O157 infections from 1996 to 1998 are unclear. Additional surveillance data collected through FoodNet will help evaluate temporal trends in foodborne illnesses. In 1998, the FoodNet catchment area included 20.5 million persons (based on 1997 estimates), 7.7% of the U.S. population. In 1999, the catchment area will include approximately 30 million persons (1997 estimates), with Georgia initiating statewide surveillance and New York adding counties to its catchment area. Tennessee, the eighth FoodNet site, also will begin collecting data from selected counties in 1999. The 1998 final FoodNet report will include final incidence figures and other information such as illness severity. Because the sites are likely to have had increases in population since 1997 (the increase from 1996 to 1997 was 1%), the 1998 rates most likely will be slightly lower than the preliminary rates. FoodNet reports are available on the World-Wide Web at less than http://www.cdc.gov/ncidod/dbmd/foodnet/foodnet.htmgreater than . References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 03/11/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}