Key points
- Dextro-Transposition (pronounced DECKS-tro trans-poh-ZI-shun) of the Great Arteries or d-TGA is one type of congenital heart defect. Congenital means present at birth.
- This condition occurs when the heart's two main arteries carrying blood out of the heart are switched in position, or “transposed.”
- Surgical repairs for d-TGA are not a cure. People with d-TGA should schedule routine checkups with a heart doctor to stay as healthy as possible.

What it is
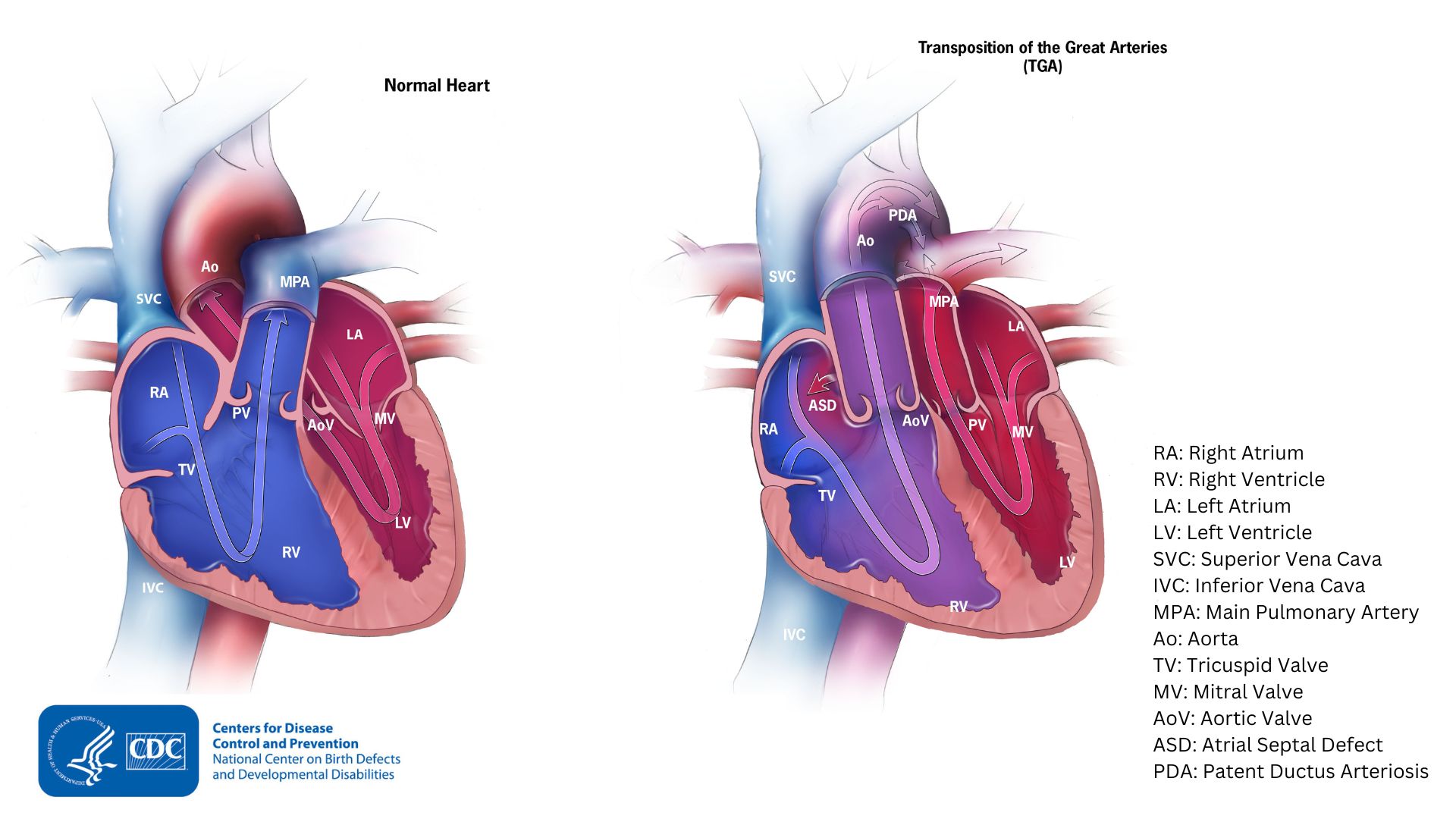
d-TGA happens when the main pulmonary artery and the aorta are switched in position, or "transposed." The main pulmonary artery and the aorta are the two main arteries that carry blood out of the heart.
In babies with d-TGA, oxygen-poor blood from the body enters the right side of the heart. But, instead of going to the lungs, the blood is pumped back out to the body through the aorta. Oxygen-rich blood from the lungs entering the heart is pumped straight back to the lungs through the main pulmonary artery.
Often, babies with d-TGA have other heart defects, such as a ventricular septal defect (VSD) or an atrial septal defect (ASD). These defects allow blood to mix so that some oxygen-rich blood can be pumped to the rest of the body. The patent ductus arteriosus (labeled PDA in the image) also allows some oxygen-rich blood to be pumped to the rest of the body.
Occurrence
About 1 in 3,957 babies in the United States are born with a d-TGA1. This means that about 928 babies are born with d-TGA each year.
Symptoms
Symptoms for d-TGA occur at birth or very soon afterwards. How severe the symptoms are will depend on whether oxygen-rich blood can get out to the rest of the body. For example, if an infant with d-TGA has an atrial septal defect (ASD), the ASD forms a passageway for some oxygen-rich blood to reach the rest of the body. Therefore, this infant with both defects may not have as severe symptoms as infants whose hearts don't have any mixing of blood.
Infants with d-TGA can have a bluish looking skin color because their blood doesn't carry enough oxygen. This condition is called cyanosis. Infants with d-TGA or other conditions causing cyanosis can have symptoms such as
- Problems breathing
- Pounding heart
- Weak pulse
- Ashen or bluish skin color
- Poor feeding
Risk factors
The causes of d-TGA among most babies are unknown. Some babies have heart defects because of changes in their genes or chromosomes. A combination of genes and other risk factors may increase the risk for AVSD. These factors can include things in a mother's environment, what she eats or drinks, or the medications she uses during pregnancy.
Diagnosis
d-TGA may be diagnosed during pregnancy or soon after the baby is born.
During pregnancy
During pregnancy, screening tests (prenatal tests) check for birth defects and other conditions. An ultrasound, a tool that creates pictures of the baby, may detect d-TGA. If the health care provider suspects d-TGA from the ultrasound, they can request a fetal echocardiogram to confirm the diagnosis. A fetal echocardiogram is a more detailed ultrasound of the baby's heart. This test can show problems with
- The structure of the heart
- The major blood vessels
- How the heart is working with this defect

After the baby is born
Because the infant with d-TGA might be bluish in color and have trouble breathing, d-TGA is usually diagnosed within the first week of life. The healthcare provider might request additional tests to confirm the diagnosis. The most common test is an echocardiogram, which is an ultrasound of the heart. An echocardiogram can show incorrect positioning of the two large arteries and any irregular blood flow. Other tests may also be used to make the diagnosis, including an electrocardiogram (EKG), chest X-rays, and other medical tests.
d-TGA can also be detected with newborn pulse oximetry screening. Newborn screening using pulse oximetry can identify some infants with d-TGA before they show any symptoms.

Treatment
Surgery is required for all babies born with d-TGA. This will help maintain, enlarge, or create openings that will deliver oxygen-rich blood to the body. Other procedures may be done before surgery.
There are two types of surgery to repair d-TGA:
Arterial Switch Operation. This is the most common procedure and it is usually done in the first month of life. It restores usual blood flow through the heart and out to the rest of the body. During this surgery, the arteries are switched to their usual positions. The pulmonary artery will be moved to arise from the right ventricle and the aorta from the left ventricle. The coronary arteries (small arteries that provide blood to the heart muscle) must also be moved and reattached to the aorta.
Atrial Switch Operation. This procedure is less commonly performed. During this surgery, the arteries are left in place. However, a tunnel (baffle) is created between the top chambers (atria) of the heart. Although this repair helps blood to go to the lungs and then out to the body, it also makes extra work for the right ventricle to pump blood to the entire body. Therefore, this repair can lead to difficulties later in life.
After surgery, medications may be needed to
- Help the heart pump better
- Control blood pressure
- Help get rid of extra fluid in the body
- Slow down the heart if it is beating too fast
If the heart is beating too slowly, a pacemaker can be used.
What to expect long-term
Infants who have surgical repairs for d-TGA are not cured. They may have lifelong complications. A child or adult with d-TGA will need regular follow-up visits with a cardiologist (a heart doctor) to monitor their progress and avoid complications or other health problems. With proper treatment, most babies with d-TGA grow up to lead healthy, productive lives.
- Stallings EB, Isenburg JL, Rutkowski RE et al; for the National Birth Defects Prevention Network. National population-based estimates for major birth defects, 2016–2020. Birth Defects Res. 2024;116(1):https://doi.org/10.1002/bdr2.2301